

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast parenchymal hamartomas comprise approximately 0.7% of all benign tumors of the female breast.(1) Arrigoni et al.(2) in 1971, first described mammary hamartomas as lesions composed of a haphazard overgrowth of mature tissues. Myoid hamartoma is a rare subtype of hamartomas that is characterized by the presence of smooth muscle cells. Only 15 cases of myoid hamartoma have been reported in the English medical literature.(3) and 2 cases have been described in the Korean literature.(4,5)
To the best of our knowledge, breast parenchymal myoid hamartoma with synchronous contralateral breast cancer has not been described. Our case manifested as a huge right breast myoid hamartoma with contralateral left invasive ductal carcinoma, which is unique.
Herein, we report the first case of myoid hamartoma of the breast parenchyma with synchronous contralateral breast cancer, and we review the relevant literatures.
CASE REPORT
A 46-yr-old woman visited our hospital due to masses in both breasts. She complained of a non-tender huge mass that had been slowly growing in her right breast for more than 3 yr, and she recently noticed a small left breast mass. Physical examination revealed a huge, firm, well circumscribed, painless mass that occupied the whole right breast and a hard, fixed, 2×2 cm mass in the periareolar area of the left breast. There were no skin changes of the breast or nipple retraction and no axillary lymphadenopathy was noted. Skin lesions, such as facial papules, trichilemmomas, oral papules, and palmoplantar keratosis were not present externally.
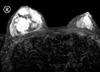
The patient had no other significant medical history and no family history of breast cancer. She had never undergone a breast examination, such as mammography or ultrasonography. An ultrasound examination showed a huge well-defined, heterogeneous echoic mass in the right breast and a 2×1.4 cm ill-defined, lobular hypoechoic mass in the periareolar area of the left breast. We performed ultrasound-guided core needle biopsy for both breast masses. Results revealed a stromal proliferative lesion of the right breast and an invasive ductal carcinoma of the left breast. A breast MRI showed a 9.2×7.2×7.1 cm mixed signal intensity lesion with variable enhancement in the right breast and a 2.1×1.9×1.5 cm oval heterogeneously early enhancing mass in the periareolar area of the left breast (Figure 1). The patient underwent subcutaneous mastectomy of the right breast and breast conserving surgery with axillary lymph node dissection of the left breast.
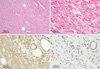
The right breast tumor grossly presented as a single, well-demarcated, firm, incompletely encapsulated mass with a smooth external surface. Microscopically, the tumor was exclusively composed of stromal elements. In the peripheral portion of the tumor, the stromal component intermingled with adipose and glandular tissue (Figure 2A). The stromal elements consisted primarily of spindle-shaped cells with eosinophilic cytoplasm and elongated cigar-shaped nuclei, and the cells were aggregated in small fascicles (Figure 2B). Nuclear pleomorphism and mitoses were not present. Immunohistochemically, the stromal spindle cells were strongly positive for smooth muscle actin but they did not express CD34, the S-100 protein, or cytokeratin (Figure 2C). Ductal epithelial cells and stromal spindle cells showed nuclear positivity for the estrogen receptor, progesterone receptor, and phosphatase and tensin homolog deleted on chromosome ten (PTEN) (Figure 2D).
These microscopic and immunohistochemical findings indicated that the spindle cells in the stroma were smooth muscle cells. The ductal epithelial cells and stromal spindle cells showed nuclear positivity for the estrogen and progesterone receptors, and PTEN. We did not perform PTEN mutation study. Invasive ductal carcinoma was identified in the contralateral breast.
These histopathologic and immunohistochemical findings indicated that the case was a myoid hamartoma of the right breast parenchyma with a synchronous invasive ductal carcinoma of the left breast.
After operation, the patient was discharged without significant complications. Two years after surgery, the patient is doing well without recurrence or metastasis.
DISCUSSION
Myoid hamartomas of the breast are a rare subtype of mammary hamartomas in which a significant smooth muscle component is identified within the stroma of the lesion. These hamartomas have been reported to constitute approximately 0.7% of all benign breast neoplasms and their main characteristic is the variety of tissues they contain.(1) Myoid hamartomas may contain both adipose and fibrous tissues in different proportions.
There are several theories about the origin of myoid differentiation. Some authors have suggested a metaplastic process from the myoepithelium as the origin of the tumor, while others have proposed that the muscle cells originate from stromal myofibroblasts or from the wall of indigenous vessels. Another theory involves differentiation of a stromal cell that can develop into adipose tissue, smooth muscle, or even cartilage, and this may explain the variety of constituents seen in breast stromal tumors, which are characterized by an impressive heterogeneity.(6)
Clinically, myoid hamartomas are usually soft, mobile, well defined masses and they differ only slightly in texture from the surrounding breast parenchyma. Because of this clinical feature, they can be misdiagnosed as fibroadenomas. The typical mammographic findings consist of a well circumscribed lesion containing both fat and soft tissue, surrounded by a thin radiopaque capsule.(7) Although mammography and a core biopsy can be diagnostic in most cases, when the diagnosis of a rare tumor like mammary hamartoma is suspected, excisional biopsy and an immunohistochemical study should be performed to make the definite diagnosis.(8)
Microscopically, these lesions are composed of a mixture of smooth muscle, fibrous stroma, and adipose tissue in varying proportions. Immunohistochemical results always contribute to a differential diagnosis. Immunohistochemical staining shows that most myoid hamartomas are positive for smooth muscle actin, desmin, caldesmon, and vimentin, but they may be negative for cytokeratin and the S-100 protein. In the present case, all histopathologic and immunohistochemical findings indicated that the mass was a myoid hamartoma. The histopathologic differential diagnosis for myoid hamartoma of the breast includes primary leiomyoma and leiomyosarcoma with a striking fascicular arrangement of smooth muscle cells and a lack of epithelioid features.(9) Neoplastic changes in mammary hamartomas are exceedingly rare. Mathers and Shrimankar(10) in 2004, reported a case with lobular neoplasia within a myoid hamartoma of the breast. Cowden syndrome, also known as multiple hamartoma syndrome, is frequently associated with a variety of malignancies, such as breast, thyroid and endometrial cancers.(11) Germline mutations in PTEN occur in 85% of patients with Cowden syndrome.(12,13) In our case, there was no clinical feature of Cowden syndrome and the ductal epithelial cells and stromal spindle cells showed nuclear positivity for PTEN immunohistochemistry.
To the best of our knowledge, this is the first case of myoid hamartoma of the breast parenchyma with synchronous contralateral breast cancer. The treatment of choice for breast hamartoma is surgical excision with tumor clear margins. If appropriate surgery is performed, the prognostic outcome is good.
In summary, myoid hamartoma of the breast parenchyma is extremely rare and frequently goes unrecognized by clinicians and pathologists because this lesion looks like other benign lesions. Awareness of myoid hamartoma of the breast parenchyma will be helpful to differentiate this benign tumor from other benign and physiologic changes in the breast.
 XML Download
XML Download