

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The goals of modern surgical treatment of breast cancer include the cure of the patients, preservation of normal breast tissues and satisfying patients' desire esthetically.(1) Breast conserving surgery (BCS) is now one of standard surgical treatment of early breast cancer patients.(2,3) In the results of National Surgical Adjuvant Breast and Bowel Project B-06 (NSABP B-06),(4) the oncologic results of BCS are equivalent to those of modified radical mastectomy (MRM). Although BCS achieved more acceptable cosmetic outcomes compared with MRM, many patients are still poorly satisfied because of the distortions of breast size and shape. Especially, small breast or inferior quadrant breast tumors showed more unfavorable cosmetic outcomes. To overcome this problem, many oncoplastic approaches were introduced; i.e. the classical mammoplastic techniques, using of local flap like a latissimus dorsi muscle flap, glandular rotation technique and so on. These oncoplastic approaches made it possible to resect larger breast tissues for margins free of tumors with achieving an esthetic goal.(5) And long-term oncologic results of BCS with plastic surgical corrections are equivalent to those of conventional BCS randomized trials.(6) Nowadays, the needs of oncoplastic surgery to improve cosmetic outcomes are more and more increasing. In this study, we examined whether or not Vicryl mesh correction is superior to conventional BCS alone for cosmesis.
METHODS
Among 56 patients who underwent breast surgery at Hallym Sacred Heart hospital and completed our questionnaire, 33 patients of them had been treated with Vicryl mesh correction and the other 23 patients conventional BCS alone. The conventional BCS is a lumpectomy or a partial mastectomy without correction of dead space. The patients were asked to complete an 3-question written survey to ascertain patient satisfaction with breast contour after surgery, postoperative pain and consistency of the breast. And patients were asked to rate their outcomes on a four point scale (1=very good, 2=good, 3=fair, 4=poor). Patient data obtained from the enrolled patients including age, body mass index (BMI), location of tumor and surface area of tumor resected. The data was collected 6 to 12 months later after surgery. The absorbable implant was made of the Vicryl mesh® (Polyglactin 910 Mesh, 26.5×21.5 cm; Ethicon, Johnson and Johnson, Somerville, USA) wrapped with the Interceed® (Oxidized regenerated cellulose, 7.6×10.2 cm; Ethicon, Johnson and Johnson, Somerville, USA). After making the Vicryl mesh into folding fan, we wrapped it with the Interceed® and sutured with Vicryl (Figure 1). And we put this absorbable implant into the dead space (Figure 2). Prophylactic antibiotics (1st generation cephalosporin) was administered for 7 days after corrective surgery. We calculated the resection area of breast tissue by long axis multiplied by short axis of removed mass.
Comparison of patients' satisfaction between conventional BCS group and Vicryl mesh group was carried out with the Pearson chi square test and analysis of cosmetic outcomes in vicryl mesh correction group was done with Kruskal-Wallis. p-values of less than 0.05 were considered statistically significant. All statistical analyses were performed using SPSS statistical software (version 14; SPSS, Chicago, USA).
RESULTS
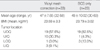
The median age of the Vicryl mesh group was 47 yr (range 32-58 yr) and that of the conventional BCS group was 49 yr (range 30-69 yr). The mean BMI of the former was 23.59±3.3 kg/m2 and that of the latter was 23.79±3.02 kg/m2. In terms of the locations of tumor in the Vicryl mesh group, upper outer quadrant (UOQ) was 57.6%, upper inner quadrant (UIQ) 30.3%, lower outer quadrant (LOQ) 3% and lower inner quadrant (LIQ) 9.1%. In the conventional BCS group, the location of tumor was, UOQ 82.6%, UIQ 4.3%, LOQ 13.0% (Table 1).
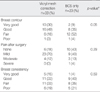
In the response of the questionnaires, 80% (23 of 33) of patients who received the Vicryl mesh correction were satisfied with their cosmetic outcomes, on the other hands only 49% (10 of 23) of patients with the BCS alone were satisfied (p=0.049, Figure 3, 4). There was no difference between two groups in postoperative pain and consistency of the breast (Table 2). In the results of clinical outcomes in the Vicryl mesh group, locations of tumor and BMI of the patients did not affect the cosmetic outcomes (Table 3). The resection area of tumor was related to the cosmesis. In cases of which resection area was less than 40 cm2, 4 of 7 patients were dissatisfied with their cosmetic outcomes. In cases of resection area more than 70 cm2, 1 of 2 patients was not satisfied. When resection area of the breast was between 40 to 70 cm2, 22 of 25 patients were satisfied (p=0.035, Table 3).
DISCUSSION
The Vicryl mesh was generally used in herniorrhaphy and other surgeries. And the safety of this absorbable implant was proved.(7) The application of this material to correct the deformity after BCS was introduced by Dr. Fukuma at Kameda hospital.(8) Several cases were reported about the insertion of the Vicryl mesh into the breast for cosmetic purposes.(9,10) We wanted to evaluate the validity of the application of Vicryl mesh as an oncoplastic procedure.
Among the 33 patients who underwent the Vicryl mesh correction, only one patient was dissatisfied. She was 46 yr old and her BMI was 23.4 kg/m2. The tumor was located in the upper outer quadreant of breast. The area, resection of tumor, was 30 cm2 (5×6 cm). She complained of focal elevated area of breast and rubber like consistency.
In 1 of 34 patients, wound infection was developed and she was excluded from this study. She had to go through chemotherapy and at 3rd cycles of adjuvant chemotherapy (5-FU, epirubicin and cyclophosphamide), she had severe neutropenia (absolute neutrophil <500/µL) and high fever. She presented continuous pain and swelling of operation site in despite of empirical antibiotics. The absorbable implant was removed and then she was recovered. We thought that severe neutropenia could cause the surgical site infection. After this case, we usually used empirical antibiotics in neutropenic patients who had undergone Vicryl mesh correction. There were no more cases of wound infection after using of prophylactic antibiotics when absolute neutrophil count less than 1,000 µL. In spite of the risk of infection, the safety of this procedure was comparable to other plastic prosthesis techniques. There were several reports that prosthesis (the polemic on silicone gel implants) techniques presented 30% of complications and 17% of the permanent expanders were removed.(11)
One of the advantages of this procedure, Vicryl mesh, is that it could be widely applicable regardless of tumor location. Besides this is very simple method. It takes just a few minutes to do this procedure. And finally, we concluded the optimal resection area of breast tissues for doing this procedure was 40-70 cm2.
Limitations of our study are that the number of patients is small and follow up period is not enough to evaluate the long term cosmetic advantages of this procedure, thus serial questionnaires need to be asked to the patients for several years and the more number of patients should be enrolled.
CONCLUSION
Recently, the surgery of breast has an esthetic goal. It is still challenging to select the appropriate plastic techniques to minimize breast deformity after BCS. Our experience with the Vicryl mesh correction showed that this absorbable implant procedure can give way excellent results in cosmesis compared with the conventional BCS. Furthermore, this procedure is very simple, safe and widely applicable regardless of location of tumor with a minimum rate of morbidity. Like this procedure, advanced volume replacement techniques can increase the rate of BCS in complex cancer cases. We suggest that this Vicryl mesh correction could be the good approach to fill in resected breast volume after BCS.





 XML Download
XML Download