

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most common female cancer worldwide, and the incidence of this malady has been continuously increasing in Korea, probably due to the westernization of life style. However, the age distribution of breast cancer patients in Korea is quite different from that of Western countries; about 60 percents of newly diagnosed breast cancer patients are premenopausal, while the premenopausal patients in Western countries constitute only 25 percents of all the breast cancer patients.(1-3)
Many studies have shown that young breast cancer patients have a worse prognosis compared with older patients.(4-7) The poor prognosis of young breast cancer patients is due to advanced disease, poor differentiation, a lesser expression of estrogen receptor (ER) or progesterone receptor (PR), a higher nuclear grade and a higher rate of tumor proliferation and tamoxifen resistance.(4,5,7-9) In 2005 at the St. Gallen consensus meetings, young age (<35 yr) was adopted as one of the important factors to categorize the risk of recurrence, and chemotherapy was considered as one of the most important strategies to improve the survival of young premenopausal breast cancer patients.(10,11)
Despite the benefit of adjuvant chemotherapy, it could provoke premature menopause and menopausal symptoms such as hot flushing, night sweats, sleep disturbance, palpitation, depression, agitation and vaginitis. Premature menopause also might cause cardiovascular morbidity, early bone mineral loss and fertility impairment.(12) However, there is insufficient information about risk factors for developing chemotherapy-induced amenorrhea (CIA) and the incidence or the pattern of resumption of menstruation after the initial development of CIA.
We conducted this study to investigate the incidence and risk factors for the occurrence of CIA and the recovery from it in young (<45 yr) breast cancer patients.
METHODS
We retrospectively studied those patients younger than 45 yr with regular menstruation and who were diagnosed with stages I to III primary invasive breast cancer from January 2003 to June 2006 at our hospital. Among them, we excluded the patients with any prior history of chemotherapy due to other cancers, a history of hysterectomy, oophorectomy or chemical ovarian suppression, an incomplete routine chemotherapy schedule, or a change of chemotherapy regimens for any reasons. The patients with poor memory of their menstrual changes were also excluded from this study. A total of 324 patients were finally analyzed.
The information about the age, stage, the clinicopathologic characteristics of the tumor, and the body mass index (BMI) at the time of diagnosis was obtained from the prospectively collected database. Information regarding the patients' menstrual cycles at diagnosis and their changes during and after chemotherapy was obtained from the medical records and one-to-one interviews with the patients.
The definition of CIA was determined as amenorrhea for more than three consecutive months at the completion of chemotherapy.(13) Recovery from CIA was defined as a start of regular menstruation after the occurrence of CIA. If irregular vaginal bleeding appeared after the development of amenorrhea, then the serum follicular stimulating hormone (FSH) level was examined. When the FSH level was 30 mIU/mL or less, then that case was classified into the recovery from CIA group.
The student t-test was used to evaluate the differences in the BMI and age at the time of diagnosis between the groups. The effects of other covariates on CIA were calculated using the Chi-square test. The risk factors for the recovery from amenorrhea were evaluated using the Kaplan-Meier method with the logistic regression model and the Cox proportional hazard model. Statistical analysis was done using SPSS software (version 14.0). All comparisons were considered significant at p-values <0.05.
RESULTS
1. Clinical characteristics of patients
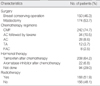
A total of 324 patients were included in this study. The mean age of the patients was 40.1 yr (range: 26-44 yr). The median follow up period was 31.3 months (range: 6-55 months) (Table 1).
The chemotherapy regimens of the 324 patients were cyclophosphamide/methotrexate/5-fluorouracil (CMF) (n=242), doxorubicin/cyclophosphamide (AC) followed by taxane (n=34), AC (n=28), anthracycline plus taxane (n=12), and 5-fluorouracil/doxorubicin/cyclophosphamide (FAC) (n=8) (Table 2). Eight (2.5%) patients received neoadjuvant chemotherapy.
Hormonal (anti-estrogen) therapy was administered to 230 (71.0%) patients, and 168 (51.9%) patients received adjuvant radiotherapy.
2. The incidence and risk factors for CIA
Of the 324 patients, 261 (80.6%) patients experienced CIA at the time of completion of chemotherapy. The age of the patient at the time of diagnosis was significantly associated with the occurrence of CIA (p<0.001), while the chemotherapy regimen, the hormonal receptor status and the BMI had no association with the initial incidence of CIA (Table 3).
3. Recovery from CIA
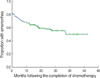
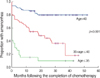
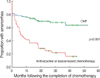
During the follow-up, 77 patients (77/261, 29.5%) resumed menstruation. The amenorrhea rates at 6, 12, 24, and 36 months after chemotherapy were 72.2%, 66.6%, 58.1%, and 55.5%, respectively (Figure 1). The patients who recovered from amenorrhea were significantly younger than those who did not (p<0.001, Figure 2). The patients treated with CMF showed the poorest recovery from amenorrhea (p<0.001, Figure 3). At 0, 6, 12, 24, and 36 months after completion of CMF, the rates of amenorrhea were 81.8%, 77.7%, 74.3%, 69.9%, and 68.0%, respectively. In contrast, the rates of amenorrhea at 0, 6, 12, 24, and 36 months after anthracycline or taxane-based chemotherapy were 78.0%, 53.7%, 41.5%, 25.3%, and 22.0%, respectively. A difference in the rates of recovery from CIA between the CMF group and the anthracycline or taxane-based group was observed for the both patient group that was <40 yr old and for the group that was ≥40 yr old (Figure 4). The hormonal receptor status, hormonal therapy, radiotherapy and BMI had no effect on the resumption of menstruation.
Age and chemotherapy regimen was evaluated using multivariate Cox proportional hazards models. On the multivariable analysis, the age of the patients and the chemotherapy regimen were significantly associated with the recovery from CIA (Table 4).
DISCUSSION
The reported incidence of amenorrhea after chemotherapy has widely varied in a range from 20% to 100%,(14-20) suggesting that there is a need for standardizing the definition of CIA. Although it has been generally reported that older premenopausal patients and the patients who were treated with a CMF regimen have shown a higher incidence of CIA due to the higher cumulative dose of cychlophosphamide,(12-15,17,18,21-23) most of the studies regarding menstrual changes after chemotherapy have not reported sufficient data to determine whether the amenorrhea is permanent or temporary. Furthermore, there has been scant data on the difference in the pattern of resumption of menstruation after initial amenorrhea according to the age of the patients and the chemotherapy regimen.
In this study, when we used the definition of CIA as described above, about 80% of women younger than 45 yr experienced amenorrhea just after completion of chemotherapy. Among them, about 30% resumed their menstruation during the follow-up. An older age was the only risk factor for the initial development of CIA. We also found that although the initial incidence of amenorrhea was not different between women who had been treated with CMF and those treated with an anthracycline or taxane-based regimen, the CMF-induced amenorrhea tends to continue or be permanent while about 80% of the anthracycline or taxane-induced amenorrhea recovered within 5 yr after the development of amenorrhea. Interestingly, this difference in the rates of resumption of menstruation was observed for the women younger than 40 yr as well as for the older women.
The prognostic impact of chemotherapy-induced menopause in young women is still controversial. A recent meta-analysis concerned with the influence of CIA on the prognosis of patients showed that the amenorrheic patients after chemotherapy had a significant survival advantage in 15 of 23 studies, but in the other studies, amenorrhea was not associated with any survival benefit.(24) Furthermore, interpretation of these trials is very difficult because the definition of amenorrhea was heterogeneous, and hormone receptor negative patients were included in many of the studies. In this study, there was no statistically significant relation between CIA and disease recurrence (data was not shown).
The role of adding ovarian suppression to the treatment for young women who remain premenopausal or who resume menstruation after chemotherapy is currently unclear. Several trials had been conducted to evaluate the role of additional ovarian suppression after chemotherapy.(25-28) Most trials have failed to demonstrate the survival advantage of adding ovarian suppression to the standard treatment such as chemotherapy plus tamoxifen. However, in the most of these trials, the menopausal status was assessed prior to chemotherapy. It is assumed that because the majority of the study population had been castrated after chemotherapy, the benefit associated with ovarian suppression might have been precluded in these trials. Ongoing phase III studies using ovarian suppression such as the Suppression of Ovarian Function Trial (SOFT) and Tamoxifen and Exemestane Trail (TEXT) might help advance current knowledge. In these trials, menopausal status was assessed only one time after chemotherapy. However, our finding that resumption of menstruation occurs in about 30% of women with CIA strongly suggests that menopausal status should be monitored for at least 2 or 3 yr after completion of chemotherapy.
CIA is very relevant issue because about 60% of the women diagnosed as breast cancer are premenopausal in Korea.(1,2) The impact of CIA on the prognosis of patients has not been well defined. The role of adding ovarian suppression to chemotherapy and tamoxifen remains unanswered. Because premature menopause is associated with considerable side effects, recognizing which subsets of patients will benefit from the induction of amenorrhea is very critical. Conducting randomized trials that would compare adding ovarian suppression to chemotherapy plus tamoxifen with chemotherapy plus tamoxifen for women who do not achieve permanent amenorrhea with chemotherapy will give us an answer to this critical question.
In the meantime, the type of adjuvant chemotherapy needs to be individualized on the base of primary needs of young women. Alkylating agent-based chemotherapy regimens, such as CMF, induce higher incidence of amenorrhea than anthracycline or taxane-based chemotherapy regimens by affecting the resting oocyte.(29) Because it has been demonstrated that the six cycles of CMF is very equivalent to 4 cycles of AC in terms of the efficacy for the adjuvant treatment of early breast cancers,(30) our finding that CMF-induced amenorrhea recovered poorly regardless of the age of patients suggests that AC may be preferable for those patients who are not married or who have plan to get pregnant. On the other hand, for those patients who are worried about the restoration of ovarian function and finishing a pregnancy, CMF might be a better choice.
CONCLUSION
The age of a patient at the time of diagnosis was the most important factor for inducing CIA. The patient treated with CMF and the older premenopausal patients recovered poorly from CIA. These results could be helpful to make decisions about the treatment strategies for premenopausal young women, and these results can also aid physicians who are attempting to balance the risk of breast cancer recurrence with the risk of ovarian failure.



 XML Download
XML Download