

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We introduce a new technique using a Vicryl® mesh made with Polyglactin 910 for breast reconstruction after performing endoscopy-assisted breast conserving surgery.
Methods
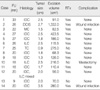
From July 2006 to July 2008, we performed endoscopiy-assisted breast surgery in 30 patients with early breast cancer. (Thirty [fourteen] patients [who] underwent endoscopy-assisted breast conserving surgery). Of the total patients, 14 underwent reconstruction procedure (volume replacement with the use of a Vicryl® mesh) and 16 underwent reconstuction without Vicryl® mesh. We were evaluated for their quality of life (QOL), the surgery-related complications and the cosmetic outcomes. Three patients were excluded from the study; two patients required mesh removal due to infection and the other patient had a total mastectomy performed due to a positive resection margin.
Results
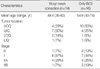
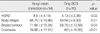
The median age of the patient was 49.4 year (range 36-60 year) and all of the patients had a diagnosis of early breast cancer (less than stage IIb). In general, the patients were satisfied with the outcome for their QOL. The patients were especially satisfied with the cosmetic outcome. The patients' satisfaction increased with longer follow-up, as compared to that for the shorter intervals. At 10 months after surgery, there was encapsulated granulation tissue within a collection of tissue fluid, as seen on ultrasonography. At 20 months after surgery, the skin and breast shape both recovered.
Figures and Tables
 | Figure 1Scheme for reconstruction using mesh. (A) Absorbable materials (polyglycolic acid mesh and oxidized regenerated cellulose) were inserted into the dead space. (B) The dead space was encapsulated by granulation and fibrous tissue in 2-3 weeks. (C) The absorbable materials had disappeared at 3 months, and the encapsulating wall with fluid prevented deformity.
|




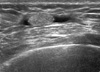 | Figure 6Sonographic finding, 10 months after operation. At 10 months after operation, there was encapsulated granulation tissue within a collection of tissue fluid on ultrasonography.
|

References
1. The Korean Breast Cancer Society. Nationwide Korean breast cancer data of 2004 using breast cancer registration program. J Breast Cancer. 2006. 9:151–161.
2. Noguchi M, Taniya T, Miyazaki I, Saito Y. Immediate transposition of a latissimus dorsi muscle for correcting a postquadrantectomy breast deformity in Japanese patients. Int Surg. 1990. 75:166–170.
3. Ohuchi N, Harada Y, Ishida T, Kiyohara H, Satomi S. Breast conserving surgery for primary breast cancer: immediate volume replace using lateral tissue flap. Breast Cancer. 1997. 4:59–65.
4. Mark RJ, Zimmerman RP, Greif JM. Capsular contracture after lumpectomy and radiation therapy in patients who have undergone uncomplicated bilateral augmentation mammaplasty. Radiology. 1996. 200:621–625.

5. Berrino P, Campora E, Santi P. Postquadrantectomy breast deformities: classification and techniques of surgical correction. Plast Reconstr Surg. 1987. 79:567–572.
6. Cooperman AM, Dinner M. The rhomboid flap and partial mastectomy. Surg Clin North Am. 1978. 58:869–873.
7. Raja MA, Straker VF, Rainsbury RM. Extending the role of breast-conserving surgery by immediate volume replacement. Br J Surg. 1997. 84:101–105.
8. Ho WS, Ying SY, Chan AC. Endoscopic-assisted subcutaneous mastectomy and axillary dissection with immediate mammary prosthesis reconstruction for early breast cancer. Surg Endosc. 2002. 16:302–306.
9. Sanuki J, Fukuma E, Wadamori K, Higa K, Sakamoto N, Tsunoda Y. Volume replacement with polyglycolic acid mesh for correcting breast deformity after endoscopic conservative surgery. Clin Breast Cancer. 2005. 6:175.
10. Nicholson RM, Leinster S, Sassoon EM. A comparison of the cosmetic and psychological outcome of breast reconstruction, breast conserving surgery and mastectomy without reconstruction. Breast. 2007. 16:396–410.
 XML Download
XML Download