

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A Mucocele-like tumor (MLT) of the breast is a rare lesion, pathologically characterized by mucin-filled cysts and extravasated mucin presented in the adjacent stroma. Although the first report of Rosen(1) described this lesion as a benign entity, an MLT has been considered as a spectrum of various pathologic lesions, including benign tumor, atypical ductal hyperplasia (ADH), ductal carcinoma in situ (DCIS), and mucinous carcinomas.(2-5) Most invasive carcinomas that arise in this setting are of the mucinous type,(6) and some authors have postulated a morphologic and biologic continuum between an MLT and mucinous carcinomas.(7) We describe a rare case of an MLT of the breast associated with columnar cell hyperplasia, DCIS and mucinous carcinoma in a 46-yr-old female.
CASE REPORT
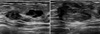
A 46-yr-old female presented with a palpable mass on left upper outer breast with no prior history of breast disease. The mammography showed a 1.8 cm equal density mass with punctuate microcalcification, a 0.9 cm size mass, and scattered microcalcifications in the upper to mid outer portion of the left breast. The ultrasonography (US) of breast showed an 1.8 cm size heterogeneously ill defined mass, a 0.9 cm size hypoechoic cystic lesion, and other multiple nodules in the left upper outer breast (Figure 1). A core needle biopsy of the associated mass lesion was subsequently performed and showed mucinous carcinoma. Magnetic resonance image (MRI) of breast showed multiple high signal intensity lesions in left upper outer breast on T2 weighted images, and dynamic contrast enhanced T1 weighted images revealed 0.6 cm and 1.7 cm size peripheral delayed enhancing lesions (Figure 2). Based on radiologic and pathologic results, we underwent mastectomy with sentinel lymph node biopsy approximately 1 month later.
In this specimen we could see an MLT associated with columnar cell hyperplasia, micro papillary type DCIS, and mucinous carcinoma on histologic examination (Figure 3). All resection margins and 3 sentinel lymph nodes were free from tumor cell invasion or metastasis, and pathologic staging of mucinous carcinoma was T1cN0M0. Immunohistochemistry showed triple positive on estrogen receptor (ER), progesterone receptor (PR), and c-erbB2. And p53 and topoisomerase II-α were negative on immunochemical stain. Then she has been treated with GnRH analogue (Goserelin Acetate 3.6 mg, s.c, monthly) and estrogen antagonists (Tamoxifen 10 mg, b.i.d, daily), after operation. The patient is well-being without evidence of local or systemic recurrence.
DISCUSSION
The pathogenesis of an MLT of the breast is still uncertain. In 1986, Rosen suggested that excess production of mucin or ductal obstruction may be contributing factors and then minor trauma is probably sufficient to cause rupture of distended cysts or ducts and extravasation of the mucin.(1) Subsequent studies have confirmed the diverse spectrum of pathologic lesions of an MLT, including benign lesions, ADH, DCIS, and mucinous carcinomas.(2-9) Some authors have postulated a morphologic and biologic continuum between an MLT and mucinous carcinomas.(7) Fine-needle aspiration cytology of benign mucocele-like tumor may be difficult to distinguish from mucinous carcinoma. It is important, therefore, to exclude the possibility of carcinoma by examining adequate tissue samples when an MLT was found in a breast biopsy. Excisional biopsy is required for an accurate diagnosis. In this case, we sampled only mucinous carcinoma through core needle biopsy specimen, and subsequent permanent histologic examination showed an MLT associated with columnar cell hyperplasia, micro-papillary type DCIS, and mucinous carcinoma (Figure 3).
Mammographic appearances of MLTs are indeterminate microcalcifications or a nodule, often containing calcifications.(10,11) In the malignant MLTs, the calcifications extended over a wider area than the calcifications in the benign MLTs.(10) but in this case, we can see the some scattered microcalcifications. Sonographic appearances of cysts with calcified or noncalcified nodules, often multiple, may suggest the diagnosis of MLTs, but the appearance does not help to differentiate between benign and malignant MLTs.(11,14)
Surgical excision is recommended for a benign MLT, and breast-conserving surgery is appropriate therapy for an MLT with carcinoma. Axillary nodal metastasis of an MLT has not been reported,(8,13) and axillary lymph node dissection may be unnecessary. Radiation therapy is indicated if a carcinoma involves margins or if extensive intraductal carcinoma is present.(2,4-8,13) In this case, she has been treated with GnRH analogue (Goserelin Acetate 3.6 mg, s.c, monthly) and estrogen antagonists (Tamoxifen 10 mg, b.i.d, daily), after operation but has not been treated with radiation therapy.
There were no appreciable differences in age, tumor size, or laterality between patients with a benign MLT or malignant one, although an MLT with carcinoma had coarse calcification more often than benign MLT.(8) Retrospective analyses have suggested that an MLT may represent a marker of a slightly increased risk for the subsequent development of invasive carcinoma when they are identified in a biopsy.(12)
We describe a case of an MLT of the breast associated with DCIS and mucinous carcinoma in a 46-yr-old female who was treated with modified radical mastectomy and hormone therapy. This case supports the concept that MLTs encompasses a spectrum of pathologic lesions including benign tumor, ADH, DCIS and mucinous carcinoma.


 XML Download
XML Download