

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
This study was performed to find the adequate number of removed lymph nodes to achieve an acceptable false-negative rate when performing sentinel lymph node biopsy for breast cancer.
Methods
A total of 179 sentinel node biopsies combined with conventional axillary lymph node dissection for breast cancer were performed between November 2003 and June 2007.
Results
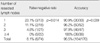
The overall identification rate of sentinel lymph node and the false negative rate of the biopsy were 95.0% and 8.1%, respectively. Yet the false negative rate of the biopsy was lowered as the number of the removed nodes was increased. Especially, the false negative rate was 0% when more than 4 lymph nodes were removed.
Figures and Tables

Table 2
The relationship between the number of resected lymph nodes and the false negative rate and the accuracy in sentinel node biopsy on permanent pathology
![]()

References
1. Fisher B, Slack NH. Number of lymph nodes examined and the prognosis of breast carcinoma. Surg Gynecol Obstet. 1970. 131:79–88.
2. McMasters KM, Tuttle TM, Carlson DJ, Brown CM, Noyes RD, Glaser RL, et al. Sentinel lymph node biopsy for breast cancer: a suitable alternative to routine axillary dissection in multi-institutional practice when optimal technique is used. J Clin Oncol. 2000. 18:2560–2566.

3. Hoar FJ, Stonelake PS. A prospective study of the value of axillary node sampling in addition to sentinel lymph node biopsy in patients with breast cancer. Eur J Surg Oncol. 2003. 29:526–531.
4. Schrenk P, Rieger R, Shamiyeh A, Wayand W. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer. 2000. 88:608–614.
5. Schwartz GF, Giuliano AE, Veronesi U. Proceedings of the consensus conference on the role of sentinel lymph node biopsy in carcinoma of the breast April 19 to 22, 2001, Philadelphia, Pennsylvania. Hum Pathol. 2002. 33:579–589.
6. Bauer TW, Spitz FR, Callans LS, Alavi A, Mick R, Weinstein SP, et al. Subareolar and peritumoral injection identify similar sentinel nodes for breast cancer. Ann Surg Oncol. 2002. 9:169–176.
7. Ikeda T, Jinno H, Fujii H, Kitajima M. Recent development of sentinel lymph node biopsy for breast cancer in Japan. Asian J Surg. 2004. 27:275–278.
8. Kim SW, Han W, Park IA, Chung JK, Yeo JS, Moon WK, et al. Prospective study of 162 sentinel lymph node biopsies in breast cancer: usefulness of ultrasonography in patients selection. J Korean Breast Cancer Soc. 2003. 6:103–108.
9. Krag D, Weaver D, Ashikaga T, Moffat F, Klimberg VS, Shriver C, et al. The sentinel node in breast cancer--a multicenter validation study. N Engl J Med. 1998. 339:941–946.
10. Smith LF, Cross MJ, Klimberg VS. Subareolar injection is a better technique for sentinel lymph node biopsy. Am J Surg. 2000. 180:434–437.
11. Zavagno G, Meggiolaro F, Rossi CR, Casara D, Pescarini L, Marchet A, et al. Subareolar injection for sentinel lymph node location in breast cancer. Eur J Surg Oncol. 2002. 28:701–704.
12. de Mascarel I, Bonichon F, Coindre JM, Trojani M. Prognostic significance of breast cancer axillary lymph node micrometastases assessed by two special techniques: reevaluation with longer follow-up. Br J Cancer. 1992. 66:523–527.
13. Hoon DS, Sarantou T, Doi F, Chi DD, Kuo C, Conrad AJ, et al. Detection of metastatic breast cancer by beta-hCG polymerase chain reaction. Int J Cancer. 1996. 69:369–374.
14. Noguchi S, Aihara T, Motomura K, Inaji H, Imaoka S, Koyama H. Detection of breast cancer micrometastases in axillary lymph nodes by means of reverse transcriptase-polymerase chain reaction. Comparison between MUC1 mRNA and keratin 19 mRNA amplification. Am J Pathol. 1996. 148:649–656.
15. McCarter MD, Yeung H, Fey J, Borgen PI, Cody HS 3rd. The breast cancer patient with multiple sentinel nodes: when to stop? J Am Coll Surg. 2001. 192:692–697.
16. Martin RC 2nd, Edwards MJ, Wong SL, Tuttle TM, Carlson DJ, Brown CM, et al. Practical guidelines for optimal gamma probe detection of sentinel lymph nodes in breast cancer: results of a multiinstitutional study. For the University of Louisville Breast Cancer Study Group. Surgery. 2000. 128:139–144.
17. Woznick A, Franco M, Bendick P, Benitez PR. Sentinel lymph node dissection for breast cancer: how many nodes are enough and which technique is optimal? Am J Surg. 2006. 191:330–333.
18. Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, Storm FK, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992. 127:392–399.
19. Morton DL, Bostick PJ. Will the true sentinel node please stand? Ann Surg Oncol. 1999. 6:12–14.
20. Nathanson SD. Will the true sentinel node please stand? Ann Surg Oncol. 1999. 6:514–516.
21. Boxen I, McCready D, Ballinger JR. Sentinel node detection and definition may depend on the imaging agent and timing. Clin Nucl Med. 1999. 24:390–394.
22. Martin RC, Fey J, Yeung H, Borgen PI, Cody HS 3rd. Highest isotope count does not predict sentinel node positivity in all breast cancer patients. Ann Surg Oncol. 2001. 8:592–597.
23. Yi M, Meric-Bernstam F, Ross MI, Akins JS, Hwang RF, Lucci A, et al. How many sentinel lymph nodes are enough during sentinel lymph node dissection for breast cancer? Cancer. 2008. 113:30–37.
24. Wong SL, Edwards MJ, Chao C, Tuttle TM, Noyes RD, Carlson DJ, et al. Sentinel lymph node biopsy for breast cancer: impact of the number of sentinel nodes removed on the false-negative rate. J Am Coll Surg. 2001. 192:684–689.
25. Kim HJ, Chang MA, Hong SJ, Lee JS, Jung MS, Kim MJ, et al. Result of sentinel lymph node biopsy using radioisotope in clinically lymph node negative breast cancer. J Breast Cancer. 2007. 10:141–146.
26. Veronesi U, Paganelli G, Galimberti V, Viale G, Zurrida S, Bedoni M, et al. Sentinel-node biopsy to avoid axillary dissection in breast cancer with clinically negative lymph-nodes. Lancet. 1997. 349:1864–1867.
27. Estourgie SH, Nieweg OE, Valdes Olmos RA, Rutgers EJ, Peterse JL, Kroon BB. Eight false negative sentinel node procedures in breast cancer: what went wrong? Eur J Surg Oncol. 2003. 29:336–340.
28. Cody HS 3rd, Fey J, Akhurst T, Fazzari M, Mazumdar M, Yeung H, et al. Complementarity of blue dye and isotope in sentinel node localization for breast cancer: univariate and multivariate analysis of 966 procedures. Ann Surg Oncol. 2001. 8:13–19.
29. Cox CE, Furman B, Dupont EL, Jakub JW, Stowell N, Clark J, et al. Novel techniques in sentinel lymph node mapping and localization of nonpalpable breast lesions: the Moffitt experience. Ann Surg Oncol. 2004. 11:222–226.
 XML Download
XML Download