

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Breast carcinoma presenting with nipple discharge is not uncommon. However, few studies have addressed the clinicopathological characteristics and optimal surgical management of breast carcinoma with nipple discharge. The aims of this study were to determine the clinicopathologic characteristics of breast carcinoma that presents with nipple discharge and the feasibility of breast conservation for these patients.
Methods
We retrospectively reviewed the medical records of the patients with breast carcinoma who presented with nipple discharge and who also underwent curative surgery at Korea Cancer Center Hospital between January 1999 and December 2003.
Results
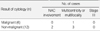
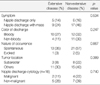
During the study periods, 40 of 1,442 (2.7%) breast cancer patients presented with nipple discharge, and among them, 28 (70%) patients were accompanied by a palpable breast mass. Their median age was 44 yr. Thirty-seven (93%) patients were treated with mastectomy and only 3 (7%) patients were treated with breast conservation. Eleven patients had ductal carcinoma in situ, 17 had stage I disease, 8 had stage II disease and 4 had stage III disease. On the pathologic evaluation, multifocality or multicentricity were found in 7 of 37 (19%) mastectomy specimens, and occult nipple-areola complex (NAC) involvement was found in 3 (8%) cases. In 23 of 37 (62%) mastectomy specimens, we didn't find any evidence of extensive disease (stage III, multicentricity or multifocality or occult NAC involvement) that may preclude breast conservation. Locoregional recurrence was not detected in any of these cases, and 37 of 40 patients are free of disease with a median follow-up of 55 months.
Conclusion
In this retrospective study, we found that 23 of 37 (62%) women with breast carcinoma associated with nipple discharge and who also underwent mastectomy had no evidence of extensive disease. Thus, we suggest that breast conservation can be done for these patients with performing careful patient selection and appropriate adjuvant therapy.
Figures and Tables



References
1. Gulay H, Bora S, Kilicturgay S, Hamaloglu E, Goksel HA. Management of nipple discharge. J Am Coll Surg. 1994. 178:471–474.
2. Newman HF, Klein M, Northrup JD, Ray BF, Drucker M. Nipple discharge. Frequency and pathogenesis in an ambulatory population. NY State J Med. 1983. 83:928–933.
3. Obedian E, Haffty BG. Breast conserving therapy in breast cancer patients presenting with nipple discharge. Int J Radiat Oncol Biol Phys. 2000. 47:137–142.

4. Miller NA, Chapman JA, Fish EB, Link MA, Fishell E, Wright B, et al. In situ duct carcinoma of the breast: clinical and histopathologic factors and association with recurrent carcinoma. Breast J. 2001. 7:292–302.
5. Cabioglu N, Krishnamurthy S, Kuerer HM, Hunt KK, Singletary SE, Meric-Bernstam F, et al. Feasibility of breast-conserving surgery for patients with breast carcinoma associated with nipple discharge. Cancer. 2004. 101:508–517.
6. The Korean Breast Cancer Society. Nationwide Korean breast cancer data of 2002. J Breast Cancer. 2004. 7:72–83.
7. Kim JS, Kim SK, Kim SI, Park BW, Lee KS. Clinical evaluation of nipple discharge. J Korean Surg Soc. 2001. 61:273–276.
8. Barreau-Pouhaer L, Le MG, Rietjens M, Arriagada R, Contesso G, Martin S, et al. Risk factors for failure of immediate breast reconstruction with prosthesis after total mastectomy for breast cancer. Cancer. 1992. 70:1145–1151.
9. Simmons RM, Brennan M, Christos P, King V, Osborne M. Analysis of nipple/areolar involvement with mastectomy: can the areola be preserved? Ann Surg Oncol. 2002. 9:165–168.
10. Cense HA, Rutgers EJ, Lopes Cardozo M, Van Lanschot JJ. Nipple-sparing mastectomy in breast cancer: a viable option? Eur J Surg Oncol. 2001. 27:521–526.
11. Wertheim U, Ozzello L. Neoplastic involvement of nipple and skin flap in carcinoma of the breast. Am J Surg Pathol. 1980. 4:543–549.
12. Kissin MW, Kark AE. Nipple preservation during mastectomy. Br J Surg. 1987. 74:58–61.
13. Laronga C, Kemp B, Johnston D, Robb GL, Singletary SE. The incidence of occult nipple-areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol. 1999. 6:609–613.
14. Lambert PA, Kolm P, Perry RR. Parameters that predict nipple involvement in breast cancer. J Am Coll Surg. 2000. 191:354–359.
15. Fisher B, Dignam J, Wolmark N, Mamounas E, Costantino J, Poller W, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998. 16:441–452.
16. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002. 347:1233–1241.
 XML Download
XML Download