

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objective
This study compared the abilities of electronic nursing records, which are based on standard nursing terminology, and paper-based nursing records to support the nursing process.
Methods
The nursing records of 38 pairs of inpatients admitted to a gynecology nursing unit were selected. The data from the paper records were obtained manually by a chart review as single statement units. The electronic records were extracted from a computerized system. The statements were categorized using the NANDA diagnosis and the modified Clinical Care Classification. Based on a semantic analysis of the components of the nursing process, the completeness of the nursing records was classified into complete and incomplete patterns according to the presence and relevancy of the assessment, the diagnosis, the intervention and the outcome.
Results
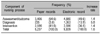
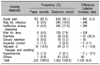
The numbers of nursing diagnoses used and the unique nursing diagnoses were both higher in the electronic records than those in the paper records. The number of statements of nursing assessments/outcomes, and nursing interventions was 1.4-fold higher in the electronic records than that in the paper records respectively. The proportion of complete patterns of the nursing process was 3.4% in the paper records and 25.7% in the electronic records.
Figures and Tables
 | Figure 1Comparison of the number of statement for pre and post implementation of an electronic nursing record system by the nursing assessment/outcome category
|
 | Figure 2Comparison of the number of statement for pre and post implementation of an electronic nursing record system by the nursing intervention category
|

Table 2
Comparison of the number of nursing statements by the component of nursing process between the paper-based nursing records and the electronic nursing records
![]()

References
1. Carpenito-Moyet LJ. Nursing care plans and documentation. 2004. 4th ed. Philadelphia: Lippincott Williams & Wilkins;3–26.
2. Chi SA, Choi KS, Park KS, Jung YK. A basic study on improvement and computerization of nursing record. J Korean Acad Nurs. 1999. 29(1):21–33.

3. Park HA, Kim JE, Cho I. Nursing diagnosis, intervention, outcome classification. 2000. Seoul: Seoul National University Press;5–24. 105–114.
4. Song MS, Kim MJ, Park YS, Lee EO, Hah YS, Han KJ, et al. Comparison of nusing activities reflected in nursing notes and in-depth interviews of nurses in an acute hospital. J Korean Acad Nurs. 2003. 33(6):802–811.
5. Lee CH, Sung YH, Jung YY, Lee JL. A study on the effects of EMR on nursing documentation. J Korean Soc Med Inform. 2000. 6(4):87–97.
6. Smith K, Smith V, Krugman M, Oman K. Evaluating the impact of computerized clinical documentation. CIN:Comput Inform Nurs. 2005. 23(3):132–138.
7. Nahm R, Poston I. Measurement of the effects of an integrated, point-of-care computer system on quality of nursing documentation and patient satisfaction. Comuters in Nursing. 2000. 18(5):220–229.
8. Larrabee JH, Boldreghini S, Elder-Sorrells K, Turner ZM, Wender RG, Hart JM, et al. Evaluation of documentation before and after implementation of a nursing information system in an acute care hospital. Computers in Nursing. 2001. 19(2):56–68.
9. Marin HF, Rodrigues RJ, Delaney C, Nielsen GH, Yan J. Building standard-based nursing information systems. Pan American Health Organization. 2001. Washington, D.C.: World Health Organization;12–15.
10. Gabrieli ER. Longitudinal electronic patient records: a challenge of our time. Computers in Nursing. 1997. 15(2):S48–S52.
11. Hardiker NR, Hoy D, Casey A. Standards for nursing terminology. J Am Med Inform Assoc. 2000. 7(6):523–528.
12. Hardiker NR, Bakken S, Casey A, Hoy D. Formal nursing terminology systems: a means to an end. J Biomed Inform. 2002. 35(5-6):298–305.
13. Bakken S, Button P, Konicek D, Matney S, McCormick K, Ozbolt JG, et al. Standardized terminologies for nursing concepts: collaborative activities in the United States. 2000. In : 7th International Congress Nursing Informatics: One Step Beyond: The Evolution of Technology and Nursing: proceedings of the NI 2000 Post Congress Workshop; Rotorua, New Zealand: International Medical Informatics Association;21–32.
14. American Nursing Association. Nursing informatics: Scope and standards of practice. 2008. Silver Spring: 1–15.
15. Park HA, Lee HS. Development of nursing information system component and interface model for integrated medical information system. 2003. Seoul: Ministry of Health and Welfare;31–66. Unpublished manuscript.
16. North America Nursing Diagnosis Association. Nursing Diagnosis: Definition and Classifications 2001-2002. 2001. 4th ed. Philadelphia: 13–207.
17. Carpenito-Moyet LJ. Nursing Diagnosis. Application to clinical practice. 2004. 10th ed. Philadelphia: Lippincott Williams & Wilkins;80–938.
18. Seoul National University Hospital. Clinical nursing process application as based on ENR. 2007. Seoul: Hyunmoon Press;33–884.
19. Saba V. Clinical Care Classification (CCC) System Manual. 2007. New York: Springer Publishing Company;103–240.
20. Nursing Text Society for the Research of Women's Health. Women's Health Nursing I, II. 2006. Seoul: Soomoonsa;1108–1120.
21. Seoul National University Hospital. Nursing Diagnosis and Planning. 1994. Seoul: Seoul National University Press;335–350.
22. Lee KH, Lee YS. Women's Health Nursing I, II. 2003. Seoul: Hyunmoon Press;1342–1358.
23. Cho I, Park HA. Contents analysis of paper-based nursing documents for electronic nursing record using ICNP. J Korean Soc Med Inform. 2002. 8(3):11–18.
24. Myung HJ. Analysis of nursing notes to develop an ICNP-based electronic nursing records system-Focused on general surgery patients' nursing records. [Dissertation]. 2003. Seoul National University.
25. Kim YJ, Park HA. Analysis of nursing records of cardiac-surgery patients based on the nursing process and focusing on nursing outcomes. Int J Med Inform. 2005. 74(11/12):952–959.
26. The 7-axis model of ICNP® version 1(chap 4). ICN. 2006. Retrieved December 12. Available at:
http://www.icn.ch/icnp_v1book.pdf.
27. Park SA, Lee HJ, Park SH. Development of computerized program for nursing diagnosis and Intervention linked to medical diagnosis. J Korean Nurs Adm Acad Soc. 2002. 8(2):239–248.
28. Cho I, Park HA. Development and evaluation of a terminology-based electronic nursing record system. J Biomed Inform. 2003. 36(4-5):304–312.
29. Cho I, Park HA. Evaluation of the expressiveness of an ICNP-based nursing data dictionary in a computerized nursing record system. J Am Med Inform Assoc. 2006. 13(4):456–464.
 XML Download
XML Download