

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Mycobacterium marinum is a ubiquitous water-borne organism that was first isolated in 1954 from dead fish and was identified as a human pathogen [1]. It causes infection in aquatic animals [2] as well as in humans at sites of contact with contaminated water [3]. The incidence of M. marinum infection in humans has been reported to range from 0.04 to 0.27 cases per 100,000 inhabitants [34]. The most frequent site is the skin and soft tissue of the hand [5]. Invasive infections such as tenosynovitis, arthritis, and osteomyelitis occasionally occur [6]. A few cases of disseminated infection of the lung by M. marinum have been reported in severely immunocompromised patients [78].
Here, we present a rare case of disseminated M. marinum involving both cutaneous tissue and the lung.
Case report
A 67-year-old male presented with multiple tender erythematous nodules and pustules distributed over his face and upper and lower extremities (Fig. 1A, B). The first skin lesion developed on his left hand about 8 months previously. Despite surgical drainage of his left hand with topical antibiotic treatment at a local hospital, the lesion spread to the face and upper and lower extremities. He complained of general weakness and loss of appetite. Respiratory symptoms such as cough and sputum were not evident. Generalized swelling of the upper and lower extremities was observed.
Figure 1
Photographs of multiple erythematous tender nodules and pustules (arrow) distributed over the face (A) and lower extremities (B). Computed tomography of the face showing multiple, variable-sized, peripherally enhanced, round lesions (arrow) in the subcutaneous layer (C). Computed tomography of the femur showing longitudinal tubular abscess pockets (arrow) in the subcutaneous layer of both thighs, together with fat necrosis (D).

The patient had been employed by a deep-water fishery for more than 30 years. He had been taking oral hypoglycemic agents for treatment of diabetes mellitus for 3 years. He had a history of intermittent steroid injections for treatment of arthralgia at the local hospital for the past 6 months. He recalled experiencing multiple minor skin lacerations while working but not sufficiently severe to require medical care.
On admission, the patient had a blood pressure of 90/60 mmHg, pulse rate of 68 beats/min, respiratory rate of 20/min, and a body temperature of 36.3°C. Laboratory findings were as follows: white blood cell count 12,500/mm3, hemoglobin level 11.1 g/dL, platelet count 88,000/mm3, C-reactive protein 30.15 mg/dL, blood urea nitrogen 32.6 mg/dL, creatinine 0.9 mg/dL, total protein 4.5 g/dL, and albumin 1.7 g/dL. Levels of aspartate aminotransferase, alanine transaminase, alkaline phosphatase, and lactate dehydrogenase were 45 U/L, 18 U/L, 228 U/L and 886 U/L, respectively. The serum concentration of hemoglobin A1c was 11.2%. Needle aspiration from a skin nodule on left wrist was performed for microbiological examination. Intravenous cefazolin was started as an empirical antibiotic.
On day 3 since admission, fever was detected, together with aggravation of the skin lesion on the left hand and thrombocytopenia. Two sets of blood cultures were performed, both of which showed no growth. Neutrophilia with a left shift to myelocytes and thrombocytopenia were observed in a peripheral blood smear. On day 5 since admission, pus culture from day 1 revealed methicillin-resistant Staphylococcus epidermidis; for this reason, cefazolin was changed to vancomycin. His fever persisted and he began exhibiting altered consciousness (Glasgow coma scale 13) with no improvement of the tender multiple nodules. On day 7 since admission, a rapid adrenocorticotropic hormone stimulation test was performed due to the patient’s recent history of steroid injection. The test results showed evidence of adrenal insufficiency. The patient was prescribed an oral hydrocortisone at 40 mg per day. Chest and abdomen computed tomography (CT) with enhancement was performed to identify any other fever foci. Multiple, peribronchial nodules of variable size in both lungs were observed on chest CT (Fig. 2). Other than mild fatty liver, no sign of liver cirrhosis or splenomegaly was evident on abdomen CT. The patient complained of worsening multiple arthralgias in both wrists and ankles. A three-phase bone scan revealed arthritic changes in the right shoulder, both wrists, and the right ankle. The amount of synovial fluid was insufficient for aspiration. Examination of the skin discharge from the left forearm was repeated, and acid-fast bacilli (AFB) staining and TB culture, as well as bacterial and fungal culture of sputum were performed. AFB were seen in pus and sputum samples stained with Ziehl–Neelsen. Sputum Mycobacterium tuberculosis (MTB) PCR with hybridization was negative. Skin biopsies from the left cheek and left 2nd finger were performed, and pathologic examination revealed acute suppurative inflammation and a positive Ziehl–Neelsen stain. Empirical treatment for both MTB and nontuberculous Mycobacterium (NTM) was initiated with isoniazid (300 mg once per day), rifampin (600 mg once per day), ethambutol (1,200 mg once per day), pyrazinamide (1,500 mg once per day), clarithromycin (500 mg twice per day), and intravenous cefoxitin (3 g three times per day). After 9 days of medication, the fever gradually subsided and the platelet level returned to the normal range; however, painful erythematous nodules remained. CT of the face (Fig. 1C) and both femurs (Fig. 1D) showed multiple abscess pockets in the subcutaneous layer where nodules were present. Surgical debridement of the abscess was performed under local anesthesia. NTM grew in culture of two sputum and pus samples. The organism was later identified as M. marinum using NTM-specific DNA probes (hybridization with Geno type mycobacterium CM ver. 1.0®, Hain Lifescience GmbH, Nehren, Germany). The M. marinum isolate showed resistance to doxycycline, rifampin, and trimethoprim-sulfamethoxazole. According to the microbiological results, daily medication was changed to clarithromycin (500 mg twice per day), moxifloxacin (400 mg once per day), and ethambutol (1,200 mg once per day). The patient’s symptoms gradually improved and he was discharged on day 39 since admission.
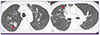
Figure 2
Chest computed tomography shows multiple variable-sized peribronchial nodules (arrow) in both upper lungs (A) and peribronchial consolidation (arrow) with perilesional ground glass opacities and interstitial thickening in the medial segment of the right middle lobe (B).
During outpatient follow-up, he continued the medications for 3 months, during which time the skin nodules disappeared and the chest radiological findings improved. However, at 3 months of follow-up, he presented to the emergency center due to an altered mental state. On chest CT, the previous peribronchial nodules were no longer visible and newly developed peribronchial consolidation and perilesional ground glass opacities were seen in the left lung and the posterior basal segment of the right lower lung. Pseudomonas aeruginosa was grown in blood culture. Streptococcus pneumoniae antigen in urine, respiratory virus, and pneumobacter PCR results were negative. The patient died during the course of the pneumonia and subsequent Pseudomonas bacteremia treatment.
Discussion
M. marinum is a major NTM that causes chronic granulomatous infections of soft tissue involving the skin and subcutaneous tissue [9]. The lesions usually appear as papules on an extremity, most frequently the forearm or hand [3], with subsequent progression to ulceration and scar formation. Most lesions are solitary, although disseminated skin lesions that resemble sporotrichosis may develop. Invasive M. marinum infection involves invasion into deeper structures, such as the synovia, bursae, and bone. Tenosynovitis is the most common manifestation of deep invasion, although septic arthritis and osteomyelitis have also been described [6]. Disseminated M. marinum infection usually occurs as a skin infection in an immunocompetent [10] or immunocompromised host [11]. In a retrospective study of 63 cases of M. marinum infection in France, most were cutaneous infections. Among them, abscess formation and invasive infection accounted for 14% and 29%, respectively [3]. So far, 5 cases of confirmed M. marinum infection with lung involvement have been reported in the literature, including this case (Table 1). Among them, disseminated M. marinum infection with pulmonary involvement occurred in a very severely immunocompromised patient, who expired during the treatment [7]. On the contrary, isolated lung involvement without cutaneous lesions have been reported in 3 immunocompetent hosts. All of the cases showed good response to the treatment [121314]. These findings expand the spectrum of disease entities caused by M. marinum. In our case, sporotrichoid skin, soft tissue lesions and multiple pulmonary nodules due to M. marinum infection were confirmed by pus and sputum culture in a patient with uncontrolled diabetes mellitus and a previous history of steroid injection. Cases of disseminated M. marinum skin infection and septic arthritis in patients receiving immunosuppressants, such as tumor necrosis factor blockers and steroids, have been reported [1516]. In our case of M. marinum infection, although an insufficient amount of synovial fluid prevented confirmation of joint involvement, worsening arthralgia over the course of the disease, joint tenderness, and swelling with multiple arthritic changes seen in bone scans suggested joint involvement. However, the possibility of other joint-involving diseases, such as osteoarthritis and rheumatoid arthritis, could not be excluded due to the limited evaluation performed. Besides lung lesions, isolation of M. marinum from blood, urine, or bone marrow has been described [1117], which suggests the possibility of hematogenous dissemination in an immunocompromised host. In our case, delayed diagnosis, underlying diabetes mellitus and use of steroids seem to have contributed to disseminated infection involving the skin, lung, and possibly the skeletal system.
Table 1
Confirmed cases of Mycobacterium marinum infection with lung involvement

| Reference | Age/Sex | Underlying disorder | Predisposing factors | Involved organ | Imaging | Diagnosis | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Present case | 67/M | DM | Use of corticosteroids | Skin, lung | Multiple peribronchial nodules | Sputum culture | CLR+MXF+ETM | Expired due to Pseudomonas bacteremia |
| [7] | 44/M | Hemophilia | None | Skin, lung, spleen, bone marrow, liver, lymph node | Diffuse infiltration | Sputum & pleural effusion culture | RIF+MIN+INH+ETM+TMP/SMX | Expired |
| AIDS | ||||||||
| [13] | 51/F | None | None | Lung | Nodular lesion with pleural retraction and segmental atelectasis | Lung biopsy tissue culture | Surgical excision and subsequent RIF+ETM | Improved |
| [14] | 39/M | None | None | Lung | Reticulonodular infiltration, bilateral hilar lymphadenopathy (sarcoidosis) | Sputum culture, Lung biopsy tissue PCR-RFLP | Corticosteroids | Improved |
| [15] | 81/M | None | None | Lung | Bilateral reticular infiltration, Pneumothorax | Sputum culture | CLR+RIF+ETM | Improved |
M, male; DM, diabetes mellitus; CLR, clarithromycin; MXF, moxifloxacin; ETM, ethambutol; AIDS, acquired immunodeficiency syndrome; RIF, rifampin; MIN, minocycline; INH, isoniazid; TMP/SMX, trimethoprim-sulfamethoxazole; PCR-RFLP, polymerase chain reaction restriction-fragment length polymorphism analysis
No definite therapeutic treatment for M. marinum infection has been developed. Monotherapy with doxycycline, minocycline, clarithromycin, or a combination of rifampin and ethambutol has been reported to be successful for treating localized skin infections [18]. In contrast, combination therapy of three or four drugs is preferred for deep-seated infections, together with a longer treatment duration [5]. In cases of invasive infection or severe cutaneous infection, surgical intervention is likely to be beneficial [36]. The intrinsic resistance of M. marinum has not been extensively investigated. Several studies have reported that M. marinum is quite susceptible to rifampin and rifabutin, and that it shows relatively high minimum inhibitory concentrations to doxycycline [319]. The M. marinum strain isolated from our patient was resistant to multiple antibiotics, including rifampin, with no prior history of antibiotic usage. The patient received combination therapy comprising clarithromycin, moxifloxacin, and ethambutol. There are few reports of drug-resistant M. marinum infection [620]. In a report of a case of osteomyelitis caused by M. marinum resistant to quinolone, doxycycline, and rifampin, the patient was treated with azithromycin and trimethoprim/sulfamethoxazole according to susceptibility test results for 9 months, together with repeated incision and drainage [6]. A case of cutaneous infection caused by M. marinum resistant to doxycycline and rifampin did not respond to doxycycline monotherapy, and the authors speculated that exposure of the aquaculture environment to antibiotics may play a role in the development of resistance in water-borne microorganisms [20]. The possibility of resistance should be taken into account when treating an infectious disease caused by a microorganism of environmental origin. Susceptibility testing is required for individualized medical therapy.
Clinicians should maintain a high index of suspicion for M. marinum when evaluating patients with a history of contact with an aquatic environment and skin lesions refractory to empirical antibiotics. Delays in diagnosis and concomitant use of an immunosuppressive agent might lead to dissemination of the infection to other organs.
 XML Download
XML Download