

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Human helminth infections, mainly due to soil-transmitted helminths (STHs), lymphatic filariasis (LF), and schistosomiasis (SCH) belong to the class of neglected tropical diseases (NTDs), and are major targets of global elimination programs. There are several NTDs against which the World Health Organization (WHO) and global funding organizations are implementing their elimination activities. However, the helminths responsible for the above three diseases are the major targets due to the number of individuals affected, their wide geographical distribution, and the potential for serious irreversible complications following infection. The main strategy of programs for the elimination of those NTDs is preventive chemotherapy (PC) employing anthelmintics, such as albendazole (ADZ) or mebendazole (MBDZ) for STHs, ADZ and diethylcarbamazine (DEC) and/or ivermectin (IVM) for LF and onchocerciasis, and praziquantel (PZQT) for SCH [1].
All ADZ, MBDZ, and PZQT tablets used by the WHO to treat endemic NTDs are donated by major pharmaceutical companies; ADZ/MBDZ is supplied by GlaxoSmithKline (gsk) and PZQT by Merck and IVM by MSD. In 2017, WHO [2] reported that 613 million tablets of ADZ were shipped to countries for the LF program, 314 million ADZ tablets and 206 million MBDZ tablets for the STH program, and 151 million tablets of PZQT for SCH (Table 1). Hundreds of millions of these anthelmintic tablets are distributed globally for this PC strategy, which requires mass drug administration (MDA) in endemic communities without individual diagnosis [2].
Table 1
Global status of donated anthelmintics distributed by WHO
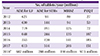
aPlanned number of treatments
WHO, world health organization; ADZ, albendazole; LF, lymphatic filariasis; STH, soil-transmitted helminths; MBDZ, mebendazole; PZQT, praziquantel.
Source: WHO/NTD 2017 [2]
![]()
MDA is only acceptable if the anthelmintics used conform to strict safety criteria. Are they really safe? The present article reviewed safety-related literature in PubMed and summarizes the contents of a safety-monitoring database for ADZ and PZQT in Korea.
Albendazole
ADZ and MBDZ are the main anthelmintics used for global deworming of STHs. ADZ is also used during preventive chemotherapy (PC) to treat LF and onchocerciasis, as well as in PC of STHs. Because ADZ is a broad spectrum anthelmintic for treatment of various helminthiases as well as STHs, it is now used for chemotherapy of toxocariasis, gnathostomiasis, echinococcosis (cystic hydatid disease), taeniasis, and cysticercosis [12]. The utility of ADZ for treatment of protozoan infections and as a candidate of anticancer chemotherapy is also being evaluated.
1. Bioactivity and pharmacokinetics
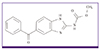
ADZ is a benzimidazole (5-propylthio-1H-benzimidazole-2-yl) carbamic acid methyl ester that was first approved as an anthelmintic for use in humans in 1982 [34]. Its vermicidal activity mainly depends on inhibiting the absorption of molecules that are critical for parasite growth; the drug’s mechanism of action is through binding to intracellular microtubules and preventing their elongation [3]. This activity preferentially affects parasites rather than the host. ADZ is relatively water insoluble and is poorly absorbed in the intestine (< 5% in humans and 50% in cattle). The degree of intestinal absorption varies greatly between species and between individuals. Eating fatty meals enhances absorption significantly, which is important for tissue parasites. Absorption is fast in humans and animals; maximum blood levels are achieved within 2–3 hours. A fraction of ADZ is metabolized in the intestinal mucosa during absorption, and ADZ that reaches the plasma after absorption is rapidly metabolized in the liver, mainly to ADZ sulfoxide and finally ADZ sulfone (the respective chemical structures are presented in Fig. 1). When a human ingests 400 mg ADZ, the Cmax of plasma ADZ sulfoxide is 0.16 mg/L; in animals the levels are much higher, due to differences in the activity of cytochrome P450 oxidases and other flavin-containing oxidases [4]. ADZ sulfoxide is the therapeutically active form, and has a t1/2 of 8–12 hours in humans. However, most of the ADZ sulfoxide is further converted by CYP2C enzymes into ADZ sulfone, which is not vermicidal [5].

One study compared the blood concentration of ADZ sulfoxide after administration of ADZ with water, fatty meals, grapefruit juice, and grapefruit juice plus cimetidine in healthy volunteers [5]. The results demonstrated a 6.5-fold higher Cmax of ADZ sulfoxide when ADZ was ingested with fatty meals, and a 3.2-fold higher Cmax in the presence of grapefruit juice compared to water. When cimetidine was combined with grapefruit juice, the Cmax was significantly decreased in comparison to grapefruit juice alone. Cimetidine inhibits CYP enzymes on the intestinal mucosa reduces gastric acid secretion, thereby reducing ADZ bioavailability by about 50% [5].
2. Adverse effects and toxicity
Previous toxicity studies reported that ADZ doses above 30–40 mg/kg/day for 4–90 days induced weight gain retardation, anemia, leukopenia, hypercholesterolemia, and proteinuria in rats [4]. Autopsy revealed enlarged livers in rats and dogs given > 40–60 mg/kg/day. Histopathologically, the centrilobular hepatocytes were enlarged, and testicular hypoplasia was noted in mice receiving 400 mg/kg/day. The oral LD50 differs according to the species; in mice it is > 3,000 mg/kg, in rats 1,320–2,400 mg/kg, and in rabbits 500–1,250 mg/kg. The results of genotoxicity and carcinogenicity studies were negative, but fetal toxicity is known to occur in rats at ADZ doses > 7.5 mg/kg/day, in rabbits between 10 and 30 mg/kg/day, and in domesticated meat animals by 10 mg/kg/day [4]. Meat from ADZ-treated domesticated meat animals is deemed fit for human consumption after a short withholding period. However, ADZ-exposed meat is not recommended for children under 24 months.
On January 9, 2018, PubMed searches for ‘ADZ toxicity’ and ‘ADZ adverse effects’ retrieved 145 and 521 articles, respectively. Only a small portion of these articles were clinical reports, and the literature regarding the enormous volumes associated with global administration of ADZ tablets is scarce [2]. ADZ is used as a single agent to treat intestinal helminths, but is frequently combined with DEC and/or IVM for the treatment of LF or onchocerciasis. Its adverse effects are relatively rare and mild in the single agent context for treatment of STHs or other intestinal helminthiases [67]. Biannual mass chemotherapy with a single dose of ADZ (400 mg) was associated with only a few cases complaining of short term abdominal discomfort from total 871 and 825 treated inhabitants in 2012 and 2013 respectively in Congo [6]. The frequency of adverse effects increases when ADZ is administered together with DEC and IVM [8]. More than half of medicated patients with LF complained, with symptoms of headache, joint pain, itching, abdominal pain, weakness, dizziness, and some objective findings such as fever, lymphadenitis, increased liver enzymes, proteinuria, hematuria, and transient lowering of blood pressure. These findings were elicited not only by ADZ, but also by combinations of anthelmintics or other drugs, and the consequential impacts of enhanced vermicidal activities. The dead bodies of filaria and microfilaria degenerate in the blood or lymph of infected hosts and, together with the drugs, this can contribute to the adverse effects reported [8].
3. Serious adverse effects
The frequency of serious adverse effects was highest when ADZ was administered at high doses for prolonged periods. The recommended dose of ADZ for the treatment of echinococcosis (hydatid cyst) in adults is 800 mg/day (two divided doses) for 1–2 months. One cohort study observing 35 children with abdominal echinococcosis in Argentina reported a mild increase in the level of liver enzymes and mild leukopenia induced by medication with ADZ 10–15 mg/kg/day for one month [9]. Cysts were inactivated in about half of the children following ADZ therapy, and the study concluded that the dose was optimal for children. However, more serious cases were reported following combined or prolonged medication, such as drug-induced psychosis by ADZ + IVM therapy [10], hemolytic anemia and kidney and brain injuries inducing acute renal failure by intravenous injection of ADZ [11], loss of body hair [12], and toxic hepatitis [131415]. One 68-year-old man reportedly died due to ADZ-induced pancytopenia [16]. He had taken 400 mg of ADZ twice a day for 16 days to treat pulmonary echinococcosis, but was admitted to hospital due to sepsis. His bone marrow was seriously suppressed, leading to pancytopenia that was not successfully treated by hospital care, and the patient died due to severe bleeding. The patient had suffered from liver cirrhosis and poor liver function; the latter condition leads to reduced metabolism in the liver, and high levels of circulating ADZ, which may inhibit the division of bone marrow hematopoietic cells. Thus, prolonged medication with ADZ requires monitoring of liver functions.
4. Anthelmintic resistance
The therapeutic failure of benzimidazole anthelmintics has been frequently reported in veterinary medicine. Because livestock are infected by various helminths, anthelmintic care is critical for their health and the economically viable production of meats or other veterinary products. ADZ resistance was noted in sheep infected by Haemonchus contortus [17]. ADZ resistance has not been confirmed in human parasites, but single nucleotide polymorphisms associated with benzimidazole resistance have been identified following genotyping of Necator americanus [18]. ADZ, fenbendazole, thiabendazole, mebendazole, oxfendazole, and ricobendazole have all been found to progressively lose their anthelmintic efficacy in livestock in Brazil [19]. This is perhaps not surprising, since ADZ and other benzimidazole derivatives have been used in huge amounts for more than 30 years, which may lead to the appearance of human-resident, drug-resistant helminths. Monitoring human parasitic helminths for the emergence of resistance thus remains a priority.
5. Anticancer efficacy
In addition to parasites, ADZ may preferentially kill cancer cells, since they can be viewed as type of ‘parasite’ in the human body. One research article proposed ADZ as a new anticancer drug candidate, since it induces oxidative stress in tumor cells, promoting DNA fragmentation and triggering apoptosis [20]. Several nanoformulations that increase bioavailability have been investigated, and some are showing promising efficacy in the treatment of parasites and tumors [2122]. More rigorous studies are expected in this emerging area of ADZ use.
6. Drug safety in pregnancy
Single agent usage of ADZ is extremely safe for MDA of STHs and LF, and WHO has approved its use during pregnancy. One Korean report described ADZ medication of 124 women during the early stages of pregnancy, and did not detect significant hazardous outcomes [23]. One meta-analysis found no difference with regard to several clinical outcome parameters among pregnant women who were treated with ADZ during the second or third trimesters [24]. Summarizing the literature, it is generally accepted that ADZ is sufficiently safe to use for MDA in areas where there is endemic STHs and LF, but that prolonged medication is not acceptable in pregnant women.
Mebendazole
MBDZ is methyl 5-benzoyl-1H-benzimidazole-2-yl-carbamate, a broad spectrum anthelmintic for human and animals (Fig. 2). MBDZ is recommended for treatment of ascariasis, hookworm infection, and trichuriasis at a dosage of 100 mg twice daily for 3 consecutive days, and for enterobiasis at a single dose of 100 mg, with a second dose of 100 mg after 2–3 weeks. The solubility of MBDZ is limited, with oral absorption of 5–10% in humans and 1–2% after a high dose. Absorption of oral MBDZ is enhanced by eating high-fat meals. The poor solubility limits its use for hydatid cyst (echinococcosis) and other tissue helminthiases. Most of the orally taken MBDZ is excreted via the feces in an unchanged form, whereas plasma MBDZ is metabolized by keto-reduction and decarbamylation of the imidazole ring [4]. The metabolites lose anthelmintic efficacy and are excreted in both the bile and urine. Individual variation of MBDZ metabolism is considerable, because of variable release and absorption rates. Co-administration of MBDZ with cimetidine leads to elevated plasma level in humans due to inhibition of first-pass cytochrome P450-mediated metabolism [4].
MBDZ was the first of several benzimidazole derivatives developed in the 1970s, whereas ADZ became more popular in 1980s. MBDZ is relatively non-toxic, but high doses may induce anemia and liver damage, as is observed with ADZ. MBDZ teratogenic in rats and mice at doses of 10 mg/kg/day, but this is not observed in other animals. MBDZ is contraindicated for pregnancy. With regard to its anthelmintic spectrum and adverse effect profile, MBDZ is almost identical to ADZ.
Praziquantel
PZQT is a pyrazinoisoquinoline with the chemical name 2-cyclohexylcarbonyl-1,2,3,6,7,11b-hexahydropyrazino (2, 1-a) isoquinolin-4-one (Fig. 3) [25]. PZQT is a broad spectrum anthelmintic in use since 1980, with activity against trematode or cestode helminthic infections of human and veterinary origin. Its bioactivity, pharmacokinetics, and clinical applications have already been discussed in detail in this journal [26].

1. Bioactivity
PZQT is a racemic mixture consisting of two enantiomers, R- and S-PZQT. An in vitro study showed that R-PZQT is essentially a vermicide agent with low toxicity, whereas S-PZQT has little anthelmintic activity, and induces toxicity [25]. The antischistosoma activity of R-PZQT is greater than that of S-PZQT, and its main metabolite, trans-4-OH-PZQT, is also effective against Schistosoma haematobium. The ED50 of PZQT is 118.1 mg/kg, while that of R-PZQT is 24.7 mg/kg and S-PZQT 127.6 mg/kg. The antischistosoma activity of PZQT is greater against female worms than it is for males. Based on the bioactivity, a pediatric formulation is currently being developed [27].
Its mode of vermicidal action is uncertain, but PZQT rapidly causes paralytic muscular contraction by increased intracellular Ca++ influx and tegumental disruption. It is hypothesized that the paralytic action of PZQT expels the worms from their primary habitat, after which the worms degenerate due to tegumental disruption [426]. Intestinal absorption is good, reaching 75–100% of the oral dose, with a tmax of 3 hours in humans. Carbohydrate-rich meals enhance PZQT absorption, but chloroquine, carbamazepine, and phenytoin may reduce its bioavailability. When coadministered with ADZ, the plasma level of PZQT is increased due to inhibition of P450 enzymes in the liver, as well as lowered metabolism. PZQT is metabolized by P450 enzymes in the liver to mono- or di-hydroxylated PZQT, and these metabolites may have weaker vermicidal activity. Clearance from the body is rapid, and occurs mainly through the urine. PZQT has no demonstrable genotoxicity, mutagenicity, carcinogenicity, or reproductive toxicity [4].
2. Target-dependent dose differences
PZQT is absorbed and cleared rapidly, as described above. The parental PZQT molecule is active, but following its metabolism, its activity drops; therefore, prolonged administration of high dose PZQT is required for tissue helminthiasis such as neurocysticercosis [26]. A single dose of 10 mg/kg PZQT is extremely effective for the treatment of intestinal trematodes or cestodes, because parental PZQT acts directly on worms in the intestine. However, a higher dose of 40 mg/kg is required for complete cure of schistosomiasis, because PZQT in the blood must act on the worm. Liver flukes (Clonorchis, Opisthorchis, Eurytrema, and Dicrocoelium) live in the intrahepatic or distal bile duct, and metabolized PZQT in the bile can expel the worms from their habitat. Thus, much higher PZQT concentration in the blood is required, and 3 doses of 25 mg/kg are recommended for treatment of liver fluke infections. Paragonimus adults reside in the middle of necrotic debris surrounded by a worm capsule, which is poorly vascularized. Therefore, a dosage of PZQT 25 mg/kg, three times per day, for 2–3 days is required to cure paragonimiasis. For neurocysticercosis, the recommended dose of PZQT is 25 mg/kgx3/day, for 7-15 days. Here, a trade-off between dosage and side effects has to be reached. Specifically, a sufficiently high level of metabolized PZQT must cross the blood brain barrier in order to treat the disease, but prolonged administration of high dose PZQT may induce more adverse effects.
3. Toxicity and adverse events
A PubMed search using the keywords ‘praziquantel adverse effect’ on January 10, 2018 retrieved 73 articles. Most articles do not describe clinical toxicity or adverse reactions, but instead focus on anthelmintic effects. In general, the frequency of adverse reactions induced by PZQT is rare; toxicities are dose-dependent and can be reduced by taking the drug alongside meals.
Rim [28] published a monograph that summarized his studies on clonorchiasis, including the use of chemotherapy with PZQT. Most of the adverse effects associated with PZQT are mild and transient, and fall into two categorized into the two categories of digestive (abdominal discomfort or pain, vomiting, and diarrhea) and neurological.(headache, drowsiness, and sleepiness) [28].
Zwang and Olliaro [29] reviewed 828 studies, which included 47 related to the efficacy of PZQT (40 mg/kg single dose) for treatment of schistosomiasis in school children. The PZQT dosage led to a 70–80% cure rate and 80–90% egg reduction rate for S. haematobium, S. mansoni, and S. japonicum infections. The most common adverse effects were drowsiness (35.7%), abdominal pain (29.9%), headache (14.1%), fatigue (13.3%), nausea (11.9%), dizziness (11.6%), weakness (11.1%), diarrhea (10.8%), muscle pain (10.0%), vomiting (7.7%), allergy (6.5%), and itching (6.1%). The incidence of any adverse event was 55.5%, which is rather high [29].
Adverse effects after PZQTmedication are produced by both drug toxicity and stimulation by dead worms in neurocysticercosis [30]. Most of the PZQT-treated patients with neurocysticercosis experienced adverse effects related to inflammation and increased intracranial pressure after death of the worms. Therefore, steroids and anticonvulsants are commonly coadministered with PZQT, although these drugs interact and can increase the frequency and severity of adverse effects. Indeed, one fatality due to increased intracranial pressure following PZQT treatment of neurocysticercosis has been reported [30].
Serious reactions are rare, but five cases of anaphylactic reaction have been reported [3031]. One 35-year old Chinese man was cared at a hospital for anaphylaxis after taking PZQT to treat clonorchiasis in 2005 [31]. Lee et al. [32] reported a 54-year old Korean woman who complained of skin rash, dyspnea, dizziness, and low blood pressure; this was the fifth case of PZQT anaphylaxis. Such an anaphylactic reaction has also been induced by antigens released from dead parasites after PZQT treatment in a murine S. japonicum infection model [33]. Table 2 summarizes the known bioavailability and safety related parameters of ADZ, MBDZ, and PZQT.
Table 2
Comparison of basic bioavailability and safety of ADZ, MBDZ, and PZQT

ADZ, albendazole; MBDZ, mebendazole; PZQT, praziquantel; STHs, soil-transmitted helminths; AE, adverse effects.
![]()
Monitoring adverse events in Korea
The Korea Institute of Drug Safety & Risk Management (KIDS) is monitoring drug safety related events and collecting nationwide reports [34]. We downloaded adverse events associated with ADZ and PZQT reported during 2006-2015 in Korea from the KIDS database. A total of 856 reports were listed with ADZ or PZQT; many overlapped with multiple complaints, whereas 256 cases were specifically associated with ADZ and 108 were associated with PZQT (Table 3). Half of the cases were not drug-related or not suitable for evaluation due to limited information, and about half were regarded as probable or possible. Only one case could be verified as an individual that was treated with ADZ and PZQT.
Table 3
Number of cases associated with ADZ- or PZQT-driven adverse events in Korea, 2006-2015
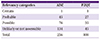
| Relevancy categories | ADZ | PZQT |
|---|---|---|
| Certain | 1 | 1 |
| Probable | 45 | 27 |
| Possible | 76 | 35 |
| Unlikely or not assessable | 134 | 45 |
| Total | 256 | 108 |
Source: Database from the Korea Institute of Drug Safety & Risk Management, 2016
ADZ, albendazole; PZQT, praziquantel.
![]()
1. Adverse events from probable or possible cases in KIDS
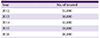
Most of the reported adverse effects were mild and transient, and subsided spontaneously and rapidly. The most frequent symptoms induced by both ADZ and PZQT were vomiting and nausea, but several other adverse effects that are often seen following anthelmintic treatment were also observed (Table 4). In Korea, ADZ is marketed freely and can be bought over the counter, whereas PZQT is accessed only under a doctor’s prescription. Currently, there is no MDA program in Korea. Based on production and marketing data generated by pharmaceutical companies, the estimated target population sizes for ADZ and PZQT treatment in Korea (2016) are 1,000,000 and 20,000, respectively. However, the number of people treated with anthelmintic medication is slowly decreasing every year. Based on the number of PZQT tablets produced by the Shin Poong Pharmaceutical Co. (Seoul, Korea), we estimate numbers of treated people in Korea (Table 5). The incidence of adverse effects should be evaluated based on numbers of consumers of the tablets. All of the adverse effects registered by the database of KIDS are described already in the literature.
Table 4
Number of casesa by reported adverse events by ADZ and PZQT in Korea, 2006-2015

aCases of probable or possible causal relations.
ADZ, albendazole; PZQT, praziquantel.
Source: Database from the Korea Institute of Drug Safety & Risk Management, 2016
![]()
2. Serious adverse effects
Although rare, serious adverse effects were recorded by KIDS for ADZ (n = 6) and PZQT (n = 2); for these cases, medical care following hospital admission was required (Table 6). One (case 1 of ADZ) was a fatality due to heart failure after administration of ADZ. The affected individual was also taking several other drugs for gastroesophageal reflux disease (GERD), which may have interfered with ADZ metabolism and thereby engendered serious adverse effects. Cimetidine, which was included in the medication for GERD, is known to inhibit ADZ metabolism [5]. The exact cause of death was marked as “unclear.” However, another serious case involved coadministration of PZQT (case 2) with famotidine and other GERD medications. Thus, administration of ADZ or PZQT to patients who are taking cimetidine or similar proton pump inhibitors is not advised.
Table 6
Cases with serious adverse effects reported to the Korea Institute of Drug Safety & Risk Management

ADZ, albendazole; F, female; GERD, gastroesophageal reflux disease; AST, aspartate transaminase; ALT, alanine transaminase; M, male; PZQT, praziquantel.
Source: Database from the Korea Institute of Drug Safety & Risk Management, 2016
![]()
Conclusion
Both ADZ and PZQT are effective and safe anthelmintics. However, coadministration with cimetidine or similar proton pump inhibitors, or treatment of patients with poor liver, heart, or kidney function can lead to serious adverse effects. Clinicians should be advised not to prescribe ADZ or PZQT to individuals with any of the above complications. Both ADZ and PZQT are not recommended for children <2 years or for pregnant women in the first trimester. The frequency of adverse events is dose-dependent, and the effects are most often seen following prolonged usage at high doses in patients with echinococcosis or neurocysticercosis. Monitoring liver functions is recommended when prolonged medication with ADZ or PZQT is prescribed. Toxicity or adverse events can not only be induced by the drugs themselves, but also by molecules that are released from dead worms after medication.
 XML Download
XML Download