

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
HACEK is an acronym comprising the first letters of the generic names of the following group of bacteria: Haemophilus parainfluenzae, Aggregatibacter actinomycetemcomitans, Aggregatibacter aphrophilus, Aggregatibacter paraphrophilus, Cardiobacterium spp., Eikenella corrodens and Kingella spp.. These organisms are fastidious Gram-negative bacteria found in the human upper respiratory and genitourinary tracts [12]. The microorganisms are generally considered to be of low virulence and to infect structurally damaged or prosthetic cardiac valves . Clinically, these cases are characterized by a subacute or chronic course and often present with embolic lesions from large vegetations and congestive cardiac failure [3]. A favorable prognosis with medical treatment [245] and a high incidence of large systemic emboli and heart failure have been reported [678]. This favorable prognosis is likely based on overestimation of positive outcomes due to considerable bias towards under-reporting unfavorable cases [9].
HACEK accounts for approximately 5–10% of native valve community-acquired endocarditis in patients who are not intravenous drug users [10] but is a rare cause (1.4%) of prosthetic valve endocarditis (PVE) [11]. Therefore, there are limited data on the clinical characteristics and outcomes of PVE caused by HACEK organisms, and the optimum treatment in patients with PVE due to HACEK is controversial. In this paper, we describe a patient who presented with HACEK PVE of the mechanical mitral valve from whom Aggregatibacter aphrophilus was isolated as the sole pathogen. We also review the English-language literature on A. aphrophilus PVE.
Case Report
A 42-year-old male presented to our hospital with fever and jaundice. He had undergone mitral valve replacement 25 years prior because of rheumatic heart disease. He had no recent history of dental manipulation or any intervention. An initial physical examination showed fever of up to 38.2°C and general weakness. All of his body's skin and sclera were yellow. Abdominal examination did not reveal any abnormalities. There was no peripheral sign of endocarditis. His white blood cell count was 22.22 × 10³/mm3, hemoglobin was 11.6 g/dL, and platelet count was 133 × 10³/mm3. The following values were also increased from normal levels: serum alanine transaminase, 47 U/L (normal range, 10–40 U/L); serum total bilirubin, 17.83 mg/dL (normal range, 0.2–1.1 mg/dL); serum direct bilirubin, 14.31 mg/dL (normal range, 0.2–0.5 mg/dL); serum alkaline phosphatase, 209 U/L (normal range, 39–108 U/L); creatinine, 1.3 mg/dL (normal range, 0.6–1.2 mg/dL); and C-reactive protein, 16.47 mg/dL (normal range, < 0.3 mg/dL). Microscopic hematuria was evident.
Abdominal computed tomography (CT) revealed a partial splenic infarction within the distal splenic artery. There was no evidence of cholangitis. A chest radiograph showed pulmonary edema. An electrocardiogram revealed atrial fibrillation. A transthoracic echocardiogram (TTE) was unremarkable but showed moderate pulmonary hypertension. A transesophageal echocardiogram (TEE) showed thrombus and vegetation in the mechanical mitral valve of a flail nature.
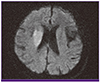
After confirmation of the presence of vegetation by TEE, treatment was started with nafcillin (2 g every 4 h) and vancomycin (1 g every 12 h), based on the assumption that Gram-negative bacteria are a rare cause of PVE and methicillin-resistant and susceptible staphylococci are most common cause of PVE. On hospital day 7, the patient showed dysarthria, left-sided weakness and drowsy mentality. Brain diffusion MRI showed acute cerebral infarction (Fig. 1). Non-sustained ventricular tachycardia appeared, and a repeat TTE showed progression of the thrombus on the mitral valve (Fig. 2). The blood culture drawn on the day of admission was reported on hospital day 9 to be positive for A. aphrophilus. This organism was confirmed by subsequent 16S rRNA sequencing. Based on the identified organism and susceptibility, antibiotic treatment was changed to intravenous ceftriaxone (2 g every 24 h) and ciprofloxacin (800 mg every 12 h) and continued for 8 weeks. On hospital day 12, the patient underwent thoracic surgery. The cultures for ordinary bacteria, fungi, and mycobacteria from surgical samples were all negative. The infected mitral valve prosthesis and left upper pulmonary vein thrombus were removed during the operation. The patient was clinically healthy and remained afebrile, but he had only partly recovered from his neurological handicap and exhibited gait disturbance at 20 months after discharge.

DISCUSSION
Our review of the English-language literature revealed 7 cases of A. aphrophilus HACEK PVE (Table 1) [11121314]. We found that the outcome of HACEK PVE was favorable, as indicated by a mortality rate of 12.5% (1/8). Fifty percent (4/8) of the patients required cardiac surgery, and 25% (1/8) experienced stroke associated with delayed blood culture reports. The major complication of A. aphrophilus PVE was stroke. Stroke is conspicuously more common in HACEK infective endocarditis (IE) (25%) compared with non-HACEK IE (17%) and was reported in cases of S. aureus endocarditis (20%) and viridans streptococcal IE (8%) in the International Collaboration on Endocarditis cohort [1516]. Mitral valve IE has been reported to be an important risk factor for stroke, as 50% (2/4) of patients with mitral valve prosthetic infection suffered a stroke compared with 0% (0/4) of patients with aortic valve prosthetic infection.
Table 1
Clinical features of eight patients with infections due to Aphrophilus aphrophilus

| Case No. [Reference] | Age/Sex | Prosthesis | Predisposing factor | Symptom Onset (day) | Complication | Diagnosisa | Surgical management | Primary antibiotic therapy (total duration of therapy) | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 [11] | 48/F | MVR | None | 1 | Cerebral infarct | Possible IE | None | Cephalothin (42 days) | Cured |
| 2 [12] | 41/F | MVR | ND | ND | None | Possible IE | Valve replacement | Penicillin (40 days) | Cured |
| 3 [12] | 70/M | AVR | ND | ND | None | Possible IE | Valve replacement | Penicillin plus streptomycin (6 weeks) | Expired |
| 4 [13] | 69/M | AVR | ND | ND | None | Possible IE | Valve replacement | Penicillin (12 weeks) | Cured |
| 5 [13] | 48/F | MVR | ND | ND | None | Possible IE | None | Penicillin plus streptomycin (7 weeks) | Cured |
| 6 [14] | 56/F | AVR | Previous IE | 60 | None | Possible IE | None | Amoxicillin and ofloxacin (34 days) | Cured |
| 7 [14] | 55/M | AVR | Previous IE | 330 | None | Possible IE | None | Cefixime and ofloxacin (56 days) | Cured |
| Present case | 42/M | MVR | None | 1 | Cerebral infarct | Definite IE | None | Ceftriaxone plus ciprofloxacin (8 weeks) | Cured |
Prompt use of antibiotics significantly reduces the incidence of emboli in patients with IE. Empirical therapy may be necessary in patients with septic shock or who show high-risk signs on presentation; however, the goal is targeted antimicrobial therapy guided by the minimum inhibitory concentration. Delayed blood culture report may be associated with stroke of HACEK PVE. Prolonged incubation may disturb the microbiologic treatment. This is important because the HACEK group organisms could be resistant to ampicillin and/or clindamycin, which may explain the therapeutic failures. Although the HACEK organisms are a rare cause of PVE, they should be considered in decision-making regarding an appropriate empirical antibiotic regimen. In conclusion, HACEK PVE is a rare disease. Increased knowledge of this rare entity may lead to early diagnosis and appropriate management.
 XML Download
XML Download