

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Bacterial meningitis persists as one of the most serious diseases in pediatric patients despite vaccine development and recent advancements in critical care techniques [1]. Failure to sufficiently treat bacterial meningitis can result in serious neurological sequelae such as hearing loss, seizures, cognitive impairment, sensory motor impairment, cerebrovascular abnormalities, subdural effusion, and other life-threatening complications [2]. Therefore, first-line therapy for bacterial meningitis in pediatric patients involves aggressive treatment with vancomycin and third-generation cephalosporins.
Studies indicate that adjunct steroid administration can reduce the likelihood of hearing loss and neurological complications, especially in cases of meningitis caused by Haemophilus influenzae type B [3, 4]. Other reports suggest that the use of steroids can inhibit the penetration of vancomycin into brain parenchyma by stabilizing the blood-brain barrier [5, 6]. Hence, adjunct steroid therapy remains controversial and is not widely used for the treatment of bacterial meningitis [7, 8]. Moreover, the utility of this treatment approach in pediatric patients is unknown, and there are no representative clinical reports describing the effects of steroid therapy on vancomycin efficacy. The purpose of this study was to verify the efficacy of combined vancomycin and steroid therapy for the treatment of culture-proven bacterial meningitis in pediatric patients.
Materials and Methods
1. Patients and treatment groups
We performed a retrospective analysis of pediatric patients with culture-proven bacterial meningitis who were admitted to Chonbuk National University Hospital between January 2005 and December 2015. This study adhered to the Declaration of Helsinki and Ethics Regulations, and was approved by the Life Science Research Ethic Council Committee at Chonbuk National University Hospital (CUH 2015-06-031-001). Included patients had confirmation of a pathogen in cerebrospinal fluid (CSF) and/or blood culture and were initially treated with vancomycin and third-generation cephalosporins. Of 86 eligible cases (Table 1), 69 were excluded because vancomycin was not used as an initial treatment, and 7 cases were excluded because the patients were neonates (age <1 month). Ultimately, 10 pediatric patients (5 boys and 5 girls) were enrolled. All patients were treated with intravenous vancomycin (60 mg/kg/day) and cefotaxime (200 mg/kg/day) as an initial empirical treatment. Additionally, all patients were positive for vancomycin-sensitive bacteria on CSF culture.
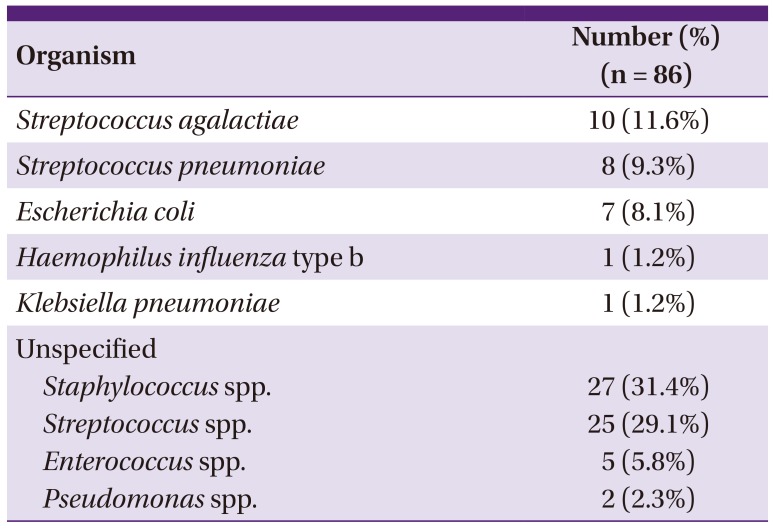
Table 1
Causative organisms of bacterial meningitis
![]()
The 10 patients were divided into 3 groups based on methylprednisolone treatment and dosage; a no steroid group, a low-dose steroid group (median dosage: 2 mg/kg/day, <5 mg/kg/day), and a high-dose steroid group (25 mg/kg/day, maximum dosage: 1 g/day for 3 days and 1 mg/kg/day thereafter). All patients had normal kidney and liver function and underwent similar adjunctive treatments for the control of fever, seizures, and intracranial pressure. The following patients were classified into the therapeutic failure group: patients with reappearance of fever [9]; those with an increased white blood cell count on follow-up CSF tap (performed in patients who showed exacerbation of clinical manifestations); those who showed positive results in follow-up CSF culture tests repeatedly. For these patients, teicoplanin was substituted with vancomycin.
2. Statistical analysis
Statistical analyses were performed using SPSS version 18.0 (SPSS, Chicago, IL, USA) and R version 3.2.1 (R Development Core Team, R Foundation, Vienna, Austria). The efficacy of antibiotics for culture-proven bacterial meningitis in pediatric patients, the vancomycin response rate according to steroid usage and neurological complications according to steroid dosage were analyzed using Fisher's exact tests. The correlation between steroid dosage and vancomycin response was analyzed using the Cochran-Armitage test. P <0.05 was the threshold for statistical significance.
Results
1. Clinical characteristics
For the 10 patients included in this study (5 boys and 5 girls), the median age was 6.5 months (range, 1–156 months) and all patients were diagnosed with bacterial meningitis by bacterial culture. Six patients were positive for Streptococcus pneumoniae and 4 patients were positive for Streptococcus agalactiae. All pathogens were vancomycin-sensitive. Six of the pathogens showed intermediate sensitivity to third-generation cephalosporins and 4 showed complete sensitivity to third-generation cephalosporins.
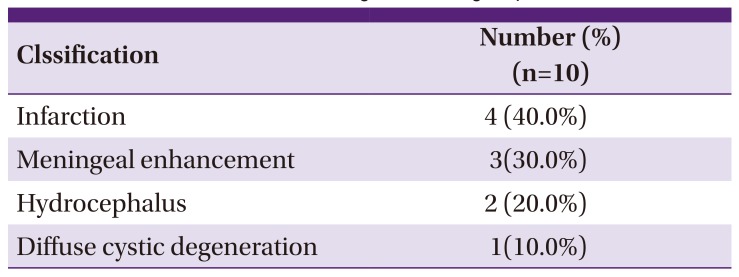
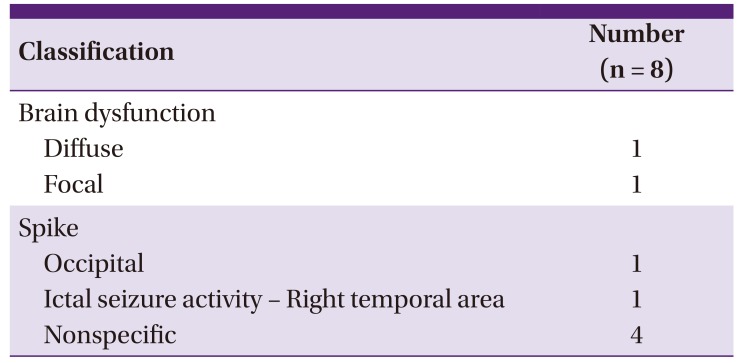
The mean white blood cell count was 2,241 ± 2,831 cells/mm3 on initial examination and 718 ± 752 cells/mm3 on follow-up examination performed within 48 h after the start of initial treatment. Almost all CSF samples had high neutrophil content (mean, 74 ± 25%). Brain magnetic resonance imaging performed on patients within 24 h of visiting the hospital identified infarction in 4 patients, meningeal enhancement in 3 patients, hydrocephalus in 2 patients, and diffuse cystic degeneration in 1 patient (Table 2). Electroencephalography performed on 8 of the 10 patients within 24 h of visiting the hospital, with the following results. Two patients showed brain dysfunction, one patient exhibited diffuse brain dysfunction, and the other presented focal brain dysfunction (Table 3). One patient showed spikes in the occipital area and the other was observed to have electrographic seizure activity in the right temporal area.
2. Antibiotics response rate
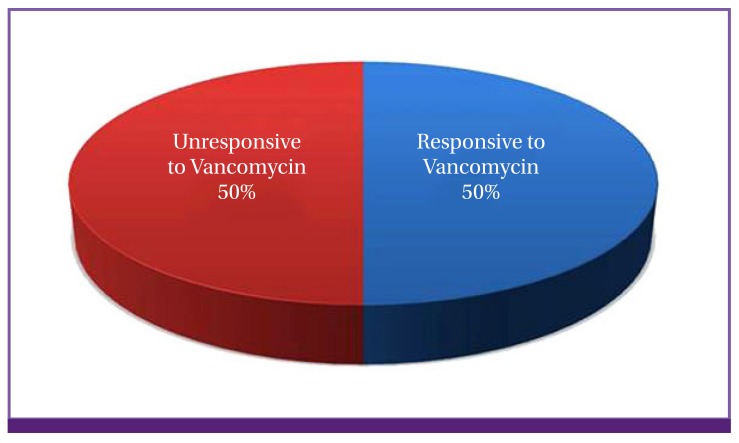
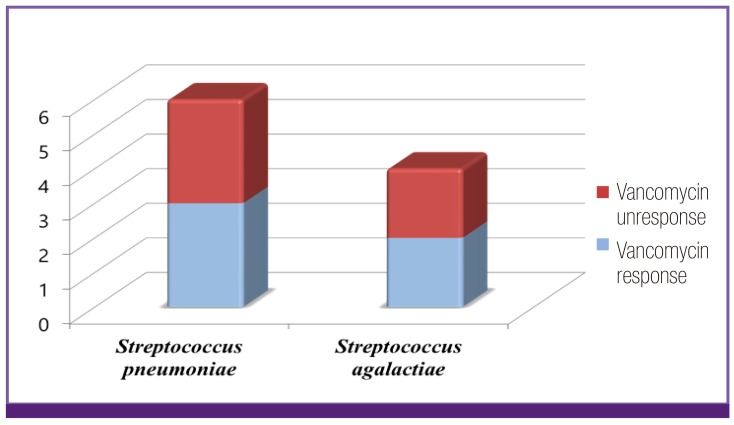
Five of the 10 patients (50.0%) responded well to vancomycin treatment (Fig. 1). The vancomycin cure rate did not differ in accordance with bacterial strain (P = 1.000, Fig. 2). The degree to which the pathogen was sensitive to third-generation cephalosporin did not affect the treatment outcome (P = 1.000).
3. The influence of concomitant steroid treatment on vancomycin efficacy
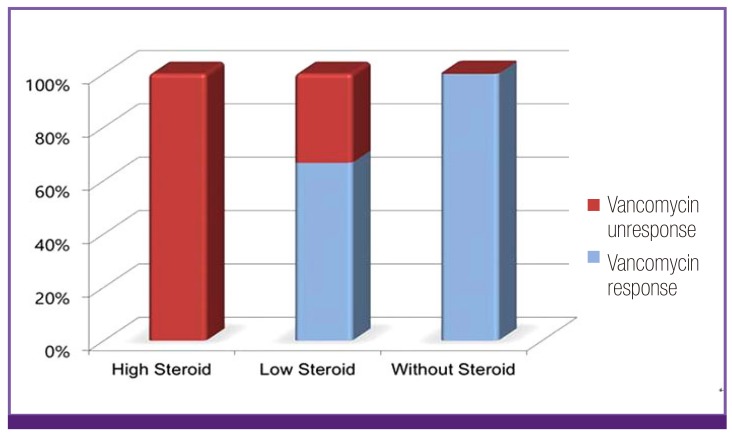
We analyzed vancomycin response rates based on the dosage of concomitant steroid treatment in order to examine effects on vancomycin efficacy. In 9 of 10 patients, methylprednisolone was used as an adjunctive therapy and was initiated concurrently with antibiotic treatment. Of the 9 patients who received steroid therapy, 4 (44.5%) responded fairly well to vancomycin while the remaining 5 (55.5%) did not respond to vancomycin at all, including all 3 patients who received high-dose steroid treatment (mean dose, 25 mg/kg/day) and 2 of 6 patients who received low-dose steroid treatment (< 5 mg/kg/day). In the 5 patients who did not respond to vancomycin, antibiotic therapy was changed to teicoplanin and steroid therapy was continued. All 5 of these patients showed good responses to combination teicoplanin and steroid therapy. Further analysis revealed that vancomycin responsiveness was significantly associated with steroid dosage (P = 0.035, Fig. 3); that is, patients receiving higher steroid dosages showed decreased responsiveness to vancomycin.
Three out of the ten patients received high steroid doses (mean dose: 25 mg/kg/day) with vancomycin and 3rd cephalosporin; however, none of them responded to antibiotics. Owing to their non-responsiveness, the patients were administered teicoplanin instead of vancomycin and steroid administration was continued. After the antibiotic was changed, all three patients responded both clinically and in follow-up CSF tap results.
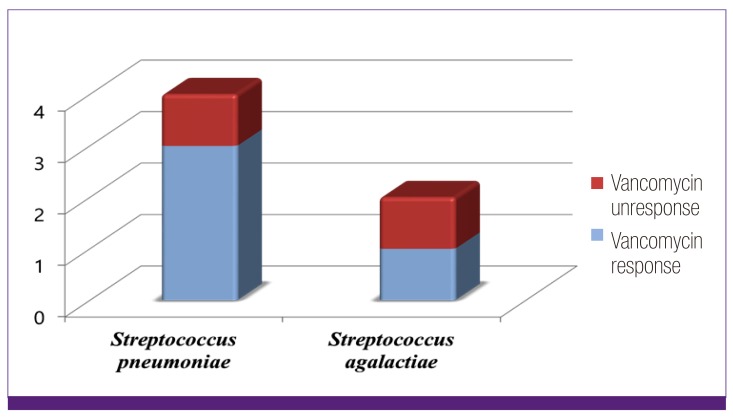
Four of the six patients (66.6%) who received less than 5 mg/kg/day of steroid responded to vancomycin; however, two (33.3%) did not respond to vancomycin and were administered teicoplanin. One patient showed reappearance of spiking fever, which subsided after having received teicoplanin instead. For the other patient, CSF cultures continued to be positive in follow-up assessments, and the patient also responded on being administered teicoplanin instead. The S. pneumoniae patient group was more responsive to vancomycin with low-dose steroid treatment compared to the S. agalactiae group (Fig. 4). However, there was no significant difference in vancomycin response rate according to bacterial strain in the low-dose steroid group (P = 1.000).
4. Neurological findings
In our cohort, 9 patients experienced seizures and changes in mental status as initial symptoms; these patients were given antiepileptic treatment in combination with initial meningitis treatment. At two months after discharge, 4 of them were taking the antiepileptic drugs prescribed to them, 1 had spastic cerebral palsy and showed language impairment, and 1 had hemiplegia and showed mental retardation. One patient required surgical shunt treatment for hydrocephalus. When the data were analyzed in terms of steroid dose and neurological complications, the low-dose steroid group had a 33.3% complication rate and the high-dose steroid group had a 100% complication rate (P = 0.167).
Discussion
Bacterial meningitis is associated with high morbidity and mortality rates and warrants prompt initial treatment with antibiotics. Currently, combination therapy is widely used, comprising vancomycin and third-generation cephalosporin. When antibiotic therapy is initiated in a timely manner, follow-up CSF cultures can be negative within the first few hours after treatment initiation [8].
Bacterial meningitis can cause serious neurological complications such as impaired mental status, cerebral edema, seizure, hearing loss, ataxia, cerebrovascular abnormality, and subdural effusion [2]. The pathophysiological mechanism of these complications involves inflammation in the CSF and subarachnoid space [10-12], which ultimately leads to cellular energy failure and death [13, 14].
Steroids can suppress inflammation in brain parenchyma and blood-brain barrier and can modulate the enhanced meningeal inflammatory response [15]. However, steroid use remains controversial because of the high incidence of recently reported complications [16] and interference with vancomycin, which can reduce the therapeutic efficacy [17-19].
High doses of steroids can stabilize the blood brain barrier (BBB), which in turn reduces its permeability and lowers the efficacy of large molecular-sized antibiotics, such as vancomycin [17]. The use of steroids dose-dependently influences the levels of key permeability regulating factors, such as angiopoietin-1 and vascular endothelial growth factor, in the cells that comprise the BBB [20-23]. Steroids can affect transcriptional regulation and have been found to increase the levels of angiopoietin-1 mRNA and protein, a strong BBB stabilizing factor, and decrease the levels of vascular endothelial growth factor mRNA and protein, which is a strong permeabilizing factor, in brain astrocytes and pericytes [24]. Thus, steroids can stabilize the BBB, thereby preventing vancomycin from penetrating the CSF, and significantly decrease the antibiotic response, especially at high doses.
Consistent with this idea, we identified dose-dependent steroid effects on vancomycin treatment efficacy in our pediatric cohort. Whereas the low-dose steroid group had a 66.6% response rate to vancomycin, the high-dose steroid group was non-responsive. Importantly, patients who were non-responsive to vancomycin therapy responded to teicoplanin co-administered with an identical steroid regimen. Similarly, Fernandez et al. [25], using a rabbit model of bacterial meningitis, reported that administration of vancomycin with a steroid was associated with therapeutic failure, whereas the use of teicoplanin with a steroid was not, despite penetration of both glycopeptides into the CSF being significantly reduced. Although the authors did not provide a complete explanation or identify possible mechanisms underlying this phenomenon, our study corroborates the observation of clinical improvement after changing the antibiotic regimen from vancomycin to teicoplanin.
The present study had some limitations. First, we included a small number of patients, such that a larger-scale study is needed to verify our results. Second, our study is limited by a retrospective design; we were not able to ensure the consistency of patient status prior to the start of treatment. Third, we did not measure levels of vancomycin in serum or CSF in our study. Despite these limitations, this study demonstrated that steroids, especially in high doses, may impair the effectiveness of vancomycin for the treating bacterial meningitis in pediatric patients. Therefore, physicians need to be more cautious with maintaining steroid therapy and the use of steroids should be decided depending on the patient's condition.
 XML Download
XML Download