

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Cytomegalovirus (CMV) remains the most important infectious agent associated with significant morbidity and occasional mortality following solid organ transplantation [1]. CMV infection is common after kidney transplantation (KT), especially up to 100 days post-KT [2–4]. Factors that influence the development of CMV infection include the CMV serostatus of the recipient and donor, the use of lymphocyte-depleting agents, immunosuppression level, and donor type (living or deceased) [5–8]. During symptomatic CMV infection, kidney transplant recipients may experience prolonged fever, leukopenia, diarrhea, hepatitis, colitis, or allograft injury. KT recipients have an increased susceptibility to opportunistic infections, an increased risk of acute rejection episodes, diminished graft survival, a higher incidence of chronic allograft nephropathy, and diminished patient survival rate [79].
Currently, the therapy for CMV infection varies among different centers; however, two strategies are acceptable according to the international guidelines: universal prophylaxis and pre-emptive therapy [910]. Universal prophylaxis involves the administration of antiviral medication to all patients or a subset of at-risk patients. Antivirals are started usually in the immediate post-kidney transplant period and continued for 3 to 6 months [10]; however, under this strategy, antiviral-resistant CMV infection in solid organ transplant recipients has been increasingly reported [11]. For pre-emptive therapy, patients are monitored regularly for CMV infection, and therapy is initiated once active viral replication is evident. Under the pre-emptive therapy guidelines, treatment is continued until two consecutive negative antigenemia assay results are obtained. Patients with CMV infection should receive intravenous ganciclovir or oral valganciclovir for a minimum of 14 days until resolution of symptoms [1213].
Pre-emptive therapy utilizes a variety of tests for detection of CMV pp65 antigen, DNA, or mRNA to diagnose and monitor therapeutic responses to CMV infection [1]. Test selection depends on many factors, including available resources, technical expertise, and the required turn-around time and cost [1415].
This study aimed to describe the occurrence, the main clinical features observed during CMV infection, and the optimum antigenemia assay cutoff associated with symptomatic CMV infection among patients submitted to renal transplantation.
Materials and Methods
1. Patients
This was a cohort study on kidney transplant recipients at a university hospital in Salvador city, Bahia state, Brazil. The enrolled patients received a kidney transplant between January 2012 and January 2013. The research protocol was approved by the Ethics Committee of Professor Edgard Santos University Hospital (No. 27/2009). Patients enrolled were from various cities in Bahia state, Brazil, whose population is characterized by African descent, ethnic miscegenation, and CMV seroprevalence greater than 85%.
2. CMV antigenemia assay and CMV infection surveillance
To prepare blood leukocytes for the CMV antigenemia assay, 14 mL of diluted ammonium chloride hemolysis buffer was added to 1 mL of ethylenediaminetetraacetic acid-treated venous blood. Leukocytes were washed twice with phosphate-buffered saline. After cytocentrifugation, leukocyte aliquots were mounted in a Neubauer cell chamber. The cell count was adjusted to 2 × 106 cells/mL. Two microscope slides were prepared by cytocentrifuging 100 µL of a leukocyte suspension containing 200,000 cells per slide. The slides were processed using the CMV Brite™ Turbo Kit (IQ Products, Groningen, Netherlands) according to the manufacturer's instructions. Positive results were confirmed in duplicate.
Kidney transplant recipients were monitored using the CMV antigenemia assay weekly for the first 3 months after transplantation. In addition, an assay was performed when there was unexplained fever, diarrhea, leukopenia, or thrombocytopenia, or when there was clinical suspicion of CMV infection. Pre-emptive therapy with intravenous ganciclovir (5 mg/kg for 14 days) was started in patients with >10 cells per slide.
3. Definitions
CMV infection was defined as virus isolation or detection of viral proteins (antigens) or nucleic acid of Cytomegalovirus in any body fluid or tissue specimen [16]. The positive antigenemia assay (≥1 positive cell per slide) was indicative of CMV infection.
Symptomatic infection was defined when a patient had a positive antigenemia assay result together with signs or symptoms generally related to CMV infection.
An episode of infection was defined as the period from diagnosis of infection until two consecutive antigenemia negative results with an interval of a week were obtained. Episodes were classified as occurring until 100 days after transplantation (D+100) or after D+100.
4. Statistical Analysis
Univariate analysis was conducted using the chi-square test for categorical variables and the Student´s test or the Mann–Whitney U test for continuous variables. The normal distribution of continuous variables was analyzed by the Kolmogorov–Smirnov test. A P value <0.05 was considered statistically significant. The receiver operator characteristic (ROC) curve was used to determine the optimum cutoff for identifying symptomatic infection.
Results
Of the 87 kidney transplant recipients enrolled, 55 (63.2%) developed CMV infection and 32 (36.8%) did not develop CMV infection during the post-transplantation period (Table 1). The median age of transplant patients who developed CMV infection (39 years) was significantly higher than those who did not develop CMV infection (19 years) (P = 0.001).
Table 1
Comparison between Cytomegalovirus (CMV) pp65-positive group and CMV pp65-negative group

D, donor; R, recipient. FK, tacrolimus; MMF, mycophenolate mofetil; Pred, prednisone; Aza, azathioprine; ATG, anti-thymocyte globulin.
P values by Chi-square test.
aMann–Whitney test.
bThere was no difference in age of the patients (P >0.05) and OR = 4.9.
cATG used for induction therapy or for treatment of acute rejection.
![]()
Sixty-five episodes of infection were observed; 45 patients had one episode while 10 patients had two. Twenty-two episodes (34%) were asymptomatic and in 43 episodes (66%) there were signs or symptoms related to CMV infection (Table 2). The infection was detected mainly until D+100 in 49/65 (75%) episodes, with a median of 60 days and 23 positive cells/200.000 leukocytes based on the antigenemia assay (Table 2).
Table 2
Characteristics of Patients with Cytomegalovirus (CMV) infection

aD+100, hundredth day after transplantation.
bCount of higher antigenemia assay per patient in number of positive cells/200.000 leukocytes.
![]()
There was no association between CMV infection and sex (P = 0.427), or CMV status prior to KT (P = 0.554), or initial immunosuppressive treatment (P = 0.761), or anti-thymocyte globulin use (P = 0.975) (Table 1). The risk of developing infection was 4.9 times higher among recipients from deceased donors (51/74, 69%) than recipients from living donors (4/13, 31%) (P = 0.009; OR = 4,9), with no significant age difference between the two groups (P >0.05) (Table 1).
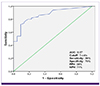
Concerning the clinical features of CMV infection, diarrhea was the most common symptom (22.6%), followed by increased creatinine serum levels (14.5%), fever (12.9%), and leukopenia (10.5%), as shown in Table 3. During follow-up of patients included in the study, no deaths were observed. The ROC curve indicated 5 cells per slide as the optimum cutoff to show signs or symptoms related to CMV infection (area under the curve (AUC) = 0.87, sensitivity = 86%, specificity = 70%, positive predictive value (PPV) = 88%, negative predictive value (NPV) = 71%), as shown in Figure 1.
Table 3
Signs and/or Symptoms during symptomatic Cytomegalovirus infection.

Adapted from Cordero et al. [3].
an = 43 episodes of symptomatic active CMV infection. All biological samples from patients with signs and symptoms presented in this table were obtained before the initiation of antiviral therapy.
![]()
Discussion
CMV infection was detected in 63.2% of the transplant recipients. Historically, the occurrence of CMV infection varies between 10% and 70% at various renal transplant centers [247]. This variation is due to several factors such as the CMV seroprevalence in the population, the serological status of the donor and the organ recipient, the type of immunosuppression used, and the method used to diagnose the infection [1].
The infection was classified as early (within 100 days after transplantation) and late (after 100 days following transplantation). Of the 65 episodes of infection observed, 75% occurred within 100 days after transplantation. This is comparable to the findings of Cordero et al., where 84% of transplant recipients showed early infection. However, it is important to note that late infection occurred in 25% of cases, which highlights the importance of continuing with monitoring after the third month following transplantation. This aspect has been highlighted in another study as well [17].
The median age of patients who had infection was higher than those who did not have infection (39 vs. 17 years). In other studies, there was no association between patient age and occurrence of active infection [313]. Other factors evaluated, such as sex, serostatus profile of the donor/recipient, use of anti-thymocyte globulin, and type of immunosuppressive therapy, did not influence the occurrence of infection. Harvala et al., also did not find a difference in the occurrence of CMV infection in transplants performed with the pre-transplant CMV status of the donor being positive and the recipient being negative, as well as the status in both recipient and donor being positive (P >0.05) [18].
In this study, it was observed that the chance of developing CMV infection was 4.9 times greater among recipients of kidneys from deceased donors than from living donors, which indicates that the use of deceased donor organ is a risk factor for infection. A similar result was reported by Schroeder et al., who observed the occurrence of symptomatic CMV infection in 49.5% of deceased donor recipients and 27% in living donor recipients (P = 0.02) [19]. These findings link the use of an organ from a deceased donor to a higher risk of occurrence of CMV infection.
CMV can cause asymptomatic or symptomatic infection, which may even develop into invasive organ infection [7]. In our study, 66% of the patients displayed symptomatic infection. Diarrhea was the most common symptom observed (22.6%), followed by increased serum creatinine levels (14.5%), fever (12.9%) and leukopenia (10.5%). Other authors observed that fever and hematological abnormalities were the most common signs or symptoms associated with CMV [6]. Cordero et al., confirmed the observation that fever is the main clinical presentation associated with CMV infection, followed by malaise, cough, leukopenia and diarrhea, in order of frequency [3]. It is noteworthy that the data on signs and/or symptoms during symptomatic Cytomegalovirus infection that are presented in Table 3 are insufficient to prove the cause-effect relationship between the symptoms presented and the CMV infection, since other factors, such as the immunosuppressive therapy, may have contributed to this relationship. More specific studies are needed to evaluate the occurrence of diarrhea, instead of fever and/or hematological abnormalities, as the main symptom associated with CMV infection.
Use of the antigenemia assay to monitor CMV infection and support pre-emptive therapy has been recommended by international guidelines for management of transplant patients [1020]. However, the cutoff point associated with the risk of symptomatic infection or that suggested for the onset of therapy has not been established, thus each center should establish and use their own cutoff point which would range from 1 to 50 positive cells per slide with 200,000 leukocytes [6].
Saracino et al., suggested that antigenemia ≥2 positive cells/200,000 leukocytes can be considered an appropriate cutoff point for starting pre-emptive therapy among renal transplant recipients [13]. In contrast, Jung et al., concluded that the therapy should be administered only to patients with ≥25 positive cells per slide [6]. For Schroeder et al., the most appropriate cutoff point for the diagnosis of symptomatic CMV infection was 4 cells per slide, and the optimal cutoff point for initiating the antiviral therapy was 10 cells per slide [19].
To evaluate this issue, a ROC curve was used to determine the cutoff point of the antigenemia assay associated with symptomatic CMV infection. The optimum cutoff was observed to be 5 positive cells/200,000 leukocytes (AUC = 0.87, sensitivity = 86% specificity = 70% PPV = 88% NPV = 71%). Based on this cutoff point, 88% of patients would have been treated before the onset of symptomatic infection, which would have reduced the occurrence of symptomatic untreated infection of 66% observed in this study to 29%. However, anticipating the cutoff point for initiation of therapy involves increasing the frequency of use of antivirals and should be viewed with caution, assessing the risks and benefits to patients.
In conclusion, the high occurrence of CMV infection observed in this study underscores the importance of implementing a protocol for monitoring and management of infection in renal transplant recipients in Bahia state, Brazil. This monitoring protocol should recognize the occurrence of early and late infection, and consider the recipient's age and the use of deceased donor organ as factors associated with increased occurrence of infection. In patients with symptomatic infection, diarrhea and elevated serum creatinine levels were the most frequent signs and symptoms. The patients present with symptomatic CMV infection once 5 positive cells/200,000 leukocytes are detected using the antigenemia assay.
 XML Download
XML Download