

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Campylobacter jejuni is one of the most common pathogens causing acute gastroenteritis in humans worldwide. It is usually transmitted through the ingestion of contaminated water or through contact with infected foods. In general, the clinical symptoms of Campylobacter enteritis include diarrhea, abdominal pain and/or fever. In <0.1% of the cases, Campylobacter infection leads to extra-intestinal complications like Guillain-Barré syndrome [1].
Most Campylobacter infections are limited to the gastrointestinal tract. Bacteremia or extra-intestinal infections are considered rare. However, several reports on Campylobacter bacteremia emphasize the importance of clinical suspicions of Campylobacter spp. due to their slow growth in culture media, and resistance against widely-used antibiotics, including cephalosporins. In this report, we elaborate on the case of a female patient with liver cirrhosis who suffered from C. jejuni bacteremia. In addition, we present a literature review of the Campylobacter bacteremia cases reported in Asian countries.
Go to : 
Case Report
A 73-year-old woman with cryptogenic liver cirrhosis (Child-Pugh score 10, class C) was hospitalized due to drowsiness, which aggravated three days before her visit to the hospital. Her initial vital signs were: blood pressure, 120/80 mmHg; heart rate, 60 beats/min; respiratory rate, 20 breaths/min; and body temperature, 36.5°C. No specific abnormalities or symptoms of infection were detected on physical examination. Initial laboratory findings showed: white blood cell (WBC) count, 5,700/mm3 (neutrophil 60.2%); hemoglobin, 10.6 g/dL; platelet count, 56,000/mm3; sodium, 144 mmol/L; potassium, 4.1 mmol/L; blood urea nitrogen (BUN), 21.2 mg/dL; and creatinine, 0.79 mg/dL. However, a liver function test showed elevated levels of aspartate transaminase (328 IU/L), alanine transaminase (259 IU/L), and alkaline phosphatase (199 IU/L). The C-reactive protein level was found to be 5.62 mg/L (normal range: 0-5 mg/L). There were no acute lesions on brain magnetic resonance imaging and a chest radiograph revealed mild cardiomegaly.
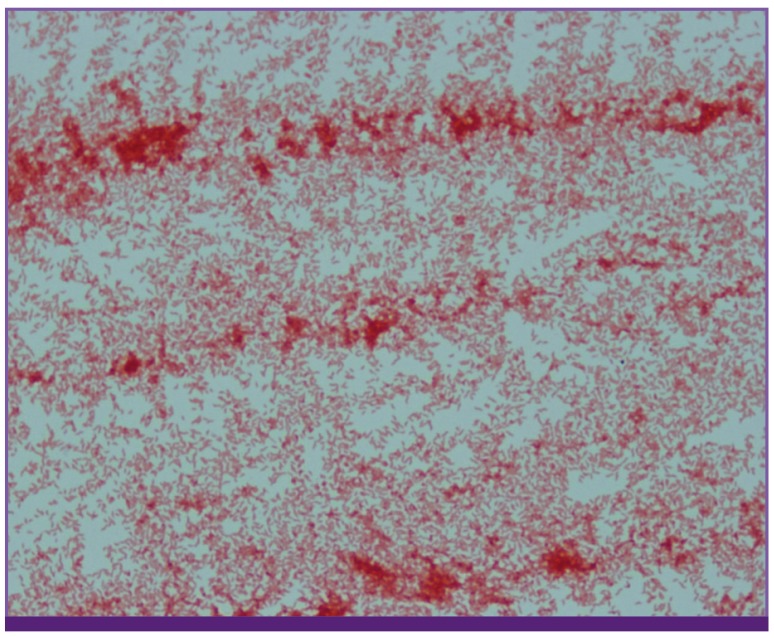
On the second day of hospitalization, a fever of 38.3°C was recorded, accompanied by chills and diarrhea. Cefotaxime (3 g/day) was administered as an empirical antibiotic to treat gastrointestinal infection. Initial fecal leukocyte tests and stool cultures yielded negative results, but after four days, a Gram-negative rod appeared in the blood culture. The patient was relieved of fever and diarrhea after two days, and cefotaxime was continued for eight days. Finally, C. jejuni was isolated in the blood culture (Fig. 1).
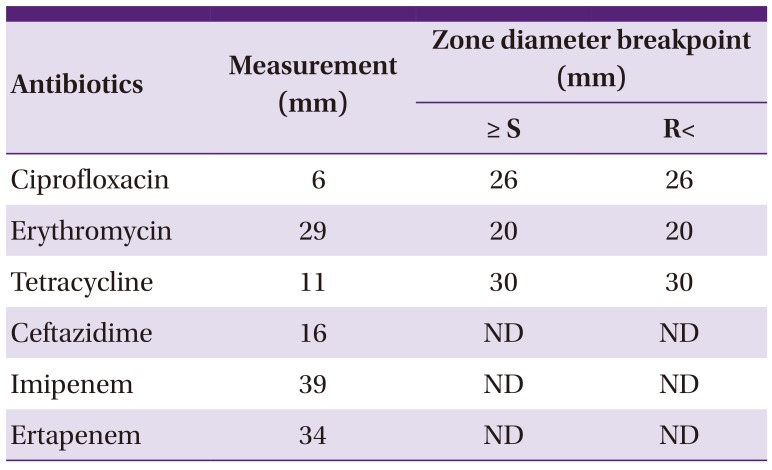
An antibiotic susceptibility test of the isolated C. jejuni was performed using the disk diffusion test, which is also called Kirby-Bauer antibiotic testing. The susceptibility was analyzed according to the epidemiological cut-off (ECOFF) values of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) [2]. The isolated C. jejuni was showen to be resistant to ciprofloxacin and tetracycline but susceptible to erythromycin. In ceftazidime (16 mm), imipenem (39 mm), and ertapenem (34 mm), relatively large zone diameters were observed; however, there is no established breakpoint of Campylobacter against these, according to the EUCAST (Table 1, Fig. 2). The total duration of hospitalization of the patient was 12 days. On discharge, the antibiotic was changed to oral azithromycin (500 mg/day), to be had for a period of five days.
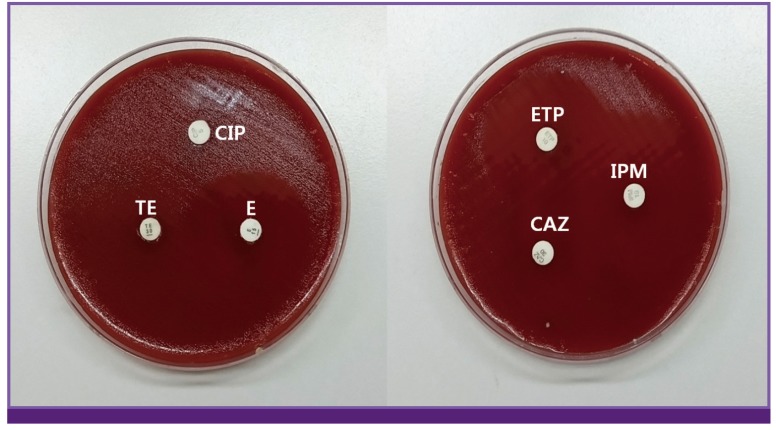 | Figure 2Antibiotic susceptibility test for isolated Campylobacter jejuni by disk diffusion method.
CIP, ciprofloxacin; TE, tetracyclin; E, erythromycin; ETP, ertapenem; IPM, imipenem; CAZ, ceftazidime.
|
Table 1
Antibiotic susceptibility of isolated Campylobacter jejuni: disk diffusion method standardized and checked by European Committee on Antimicrobial Susceptibility Testing (EUCAST)
| Antibiotics | Measurement (mm) | Zone diameter breakpoint (mm) | |
|---|---|---|---|
| ≥ S | R< | ||
| Ciprofloxacin | 6 | 26 | 26 |
| Erythromycin | 29 | 20 | 20 |
| Tetracycline | 11 | 30 | 30 |
| Ceftazidime | 16 | ND | ND |
| Imipenem | 39 | ND | ND |
| Ertapenem | 34 | ND | ND |
![]()
Go to :
Discussion
Campylobacter spp. are one of the major gastrointestinal pathogens. In the United States, 9% of all food-borne infections are caused by Campylobacter [3]. However, in South Korea, the involvement of Campylobacter in food-borne infections is considered to be low (2.5%, 2013) [4]. Campylobacter bacteremia is rare, but it should not be ignored. We presented the case of C. jejuni bacteremia in a patient with liver cirrhosis. She suffered from fever and diarrhea, but recovered with the administration of empirical antibiotics and supportive care. Campylobacter grows slowly in culture media; occasionally 72-96 hours are required for primary isolation from biological samples [5]. In this case, C. jejuni was isolated after 10 days of culture. Though Campylobacter bacteremia might resolve without antibiotic treatment in a normal host, it is important to know the local epidemiology of anti-microbial susceptibility of Campylobacter and to select appropriate empirical antibiotics to treat chronically ill patients with comorbidities.
The global burden of disease and epidemiologic characteristics of Campylobacter bacteremia in Asian countries were unknown. Thus, we reviewed the reported cases of Campylobacter bacteremia, published between 2000 and 2014 (Table 2) [16789101112131415161718]. A total of 51 Campylobacter bacteremia cases were identified (Taiwan, 25; Japan, 16; Hong Kong, 8; Singapore, 1; Thailand, 1). A majority of the patients (49/51, 96.1%) suffered from underlying diseases such as hematologic malignancy, liver disease, renal disease, or cancer, all of which can cause the deterioration of host immunity. Most of the patients had a fever (35/48, 72.9%), but diarrhea (14/48, 29.2%) and abdominal pain (9/48, 18.8%) were rare.
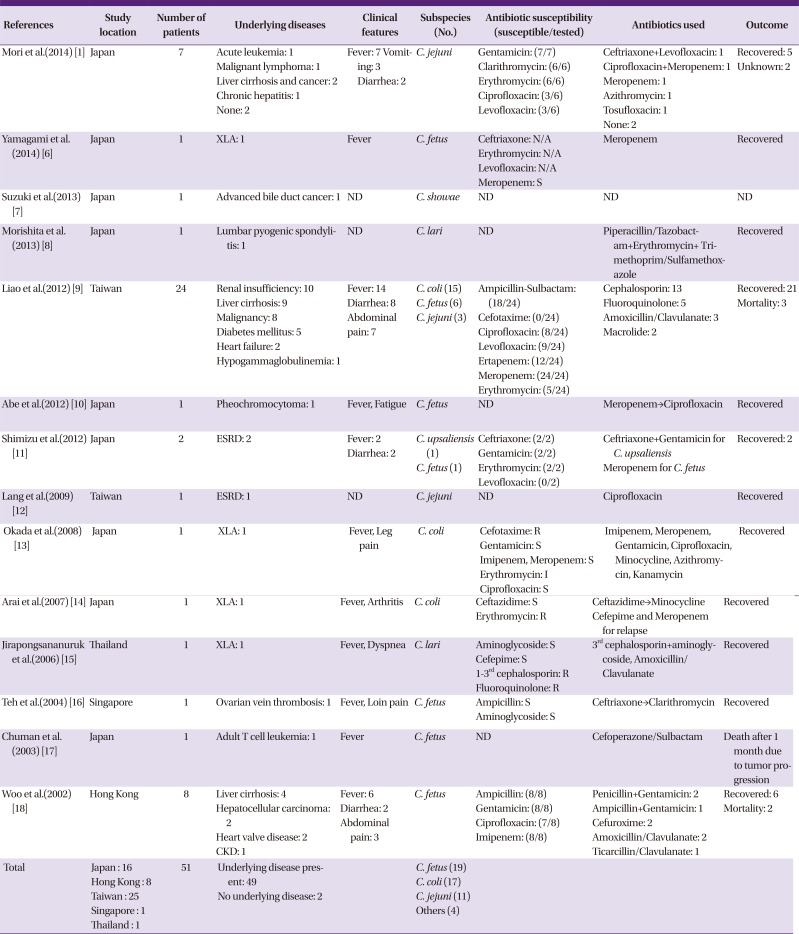
Table 2
Reported Campylobacter bacteremia cases in Asian countries during 2000-2014
| References | Study location | Number of patients | Underlying diseases | Clinical features | Subspecies (No.) | Antibiotic susceptibility (susceptible/tested) | Antibiotics used | Outcome |
|---|---|---|---|---|---|---|---|---|
| Mori et al.(2014) [1] | Japan | 7 |
Acute leukemia: 1 Malignant lymphoma: 1 Liver cirrhosis and cancer: 2 Chronic hepatitis: 1 None: 2 |
Fever: 7 Vomiting: 3 Diarrhea: 2 |
C. jejuni |
Gentamicin: (7/7) Clarithromycin: (6/6) Erythromycin: (6/6) Ciprofloxacin: (3/6) Levofloxacin: (3/6) |
Ceftriaxone+Levofloxacin: 1 Ciprofloxacin+Meropenem: 1 Meropenem: 1 Azithromycin: 1 Tosufloxacin: 1 None: 2 |
Recovered: 5 Unknown: 2 |
| Yamagami et al.(2014) [6] | Japan | 1 | XLA: 1 | Fever | C. fetus |
Ceftriaxone: N/A Erythromycin: N/A Levofloxacin: N/A Meropenem: S |
Meropenem | Recovered |
| Suzuki et al.(2013) [7] | Japan | 1 | Advanced bile duct cancer: 1 | ND | C. showae | ND | ND | ND |
| Morishita et al.(2013) [8] | Japan | 1 | Lumbar pyogenic spondylitis: 1 | ND | C. lari | ND | Piperacillin/Tazobactam+Erythromycin+Trimethoprim/Sulfamethoxazole | Recovered |
| Liao et al.(2012) [9] | Taiwan | 24 |
Renal insufficiency: 10 Liver cirrhosis: 9 Malignancy: 8 Diabetes mellitus: 5 Heart failure: 2 Hypogammaglobulinemia: 1 |
Fever: 14 Diarrhea: 8 Abdominal pain: 7 |
C. coli (15) C. fetus (6) C. jejuni (3) |
Ampicillin-Sulbactam: (18/24) Cefotaxime: (0/24) Ciprofloxacin: (8/24) Levofloxacin: (9/24) Ertapenem: (12/24) Meropenem: (24/24) Erythromycin: (5/24) |
Cephalosporin: 13 Fluoroquinolone: 5 Amoxicillin/Clavulanate: 3 Macrolide: 2 |
Recovered: 21 Mortality: 3 |
| Abe et al.(2012) [10] | Japan | 1 | Pheochromocytoma: 1 | Fever, Fatigue | C. fetus | ND | Meropenem→Ciprofloxacin | Recovered |
| Shimizu et al.(2012) [11] | Japan | 2 | ESRD: 2 |
Fever: 2 Diarrhea: 2 |
C. upsaliensis (1) C. fetus (1) |
Ceftriaxone: (2/2) Gentamicin: (2/2) Erythromycin: (2/2) Levofloxacin: (0/2) |
Ceftriaxone+Gentamicin for C. upsaliensis Meropenem for C. fetus |
Recovered: 2 |
| Lang et al.(2009) [12] | Taiwan | 1 | ESRD: 1 | ND | C. jejuni | ND | Ciprofloxacin | Recovered |
| Okada et al.(2008) [13] | Japan | 1 | XLA: 1 | Fever, Leg pain | C. coli |
Cefotaxime: R Gentamicin: S Imipenem, Meropenem: S Erythromycin: I Ciprofloxacin: S |
Imipenem, Meropenem, Gentamicin, Ciprofloxacin, Minocycline, Azithromycin, Kanamycin | Recovered |
| Arai et al.(2007) [14] | Japan | 1 | XLA: 1 | Fever, Arthritis | C. coli |
Ceftazidime: S Erythromycin: R |
Ceftazidime→Minocycline Cefepime and Meropenem for relapse |
Recovered |
| Jirapongsananuruk et al.(2006) [15] | Thailand | 1 | XLA: 1 | Fever, Dyspnea | C. lari |
Aminoglycoside: S Cefepime: S 1–3rd cephalosporin: R Fluoroquinolone: R |
3rd cephalosporin+aminoglycoside, Amoxicillin/Clavulanate | Recovered |
| Teh et al.(2004) [16] | Singapore | 1 | Ovarian vein thrombosis: 1 | Fever, Loin pain | C. fetus |
Ampicillin: S Aminoglycoside: S |
Ceftriaxone→Clarithromycin | Recovered |
| Chuman et al.(2003) [17] | Japan | 1 | Adult T cell leukemia: 1 | Fever | C. fetus | ND | Cefoperazone/Sulbactam | Death after 1 month due to tumor progression |
| Woo et al.(2002) [18] | Hong Kong | 8 |
Liver cirrhosis: 4 Hepatocellular carcinoma: 2 Heart valve disease: 2 CKD: 1 |
Fever: 6 Diarrhea: 2 Abdominal pain: 3 |
C. fetus |
Ampicillin: (8/8) Gentamicin: (8/8) Ciprofloxacin: (7/8) Imipenem: (8/8) |
Penicillin+Gentamicin: 2 Ampicillin+Gentamicin: 1 Cefuroxime: 2 Amoxicillin/Clavulanate: 2 Ticarcillin/Clavulanate: 1 |
Recovered: 6 Mortality: 2 |
| Total |
Japan : 16 Hong Kong : 8 Taiwan : 25 Singapore : 1 Thailand : 1 |
51 |
Underlying disease present: 49 No underlying disease: 2 |
C. fetus (19) C. coli (17) C. jejuni (11) Others (4) |
N/A, not applicable; ND, no data; S, susceptible; I, intermediate; R, resistant; XLA, X-liked agammaglobulinemia; TB, tuberculosis; CKD, chronic kidney disease; ESRD, end-stage renal disease.
![]()
Microbiologically, C. fetus was found to be the most common strain (19/51, 37.3%) infecting these patients, followed by C. coli (17/51, 33.3%) and C. jejuni (11/51, 21.6%). C. upsaliensis, C. showae, and C. lari were also presented in several reports (Table 2) [16789101112131415161718]. Thus, if extra-intestinal symptoms manifest in a patient and a Gram stain of the blood sample suggests the presence of a Campylobacter spp., C. fetus, C. coli, or C. jejuni infection should be considered.
Generally, third generation cephalosporins with or without aminoglycoside, macrolide monotherapy, or fluoroquinolone monotherapy were used as empirical treatments for Campylobacter infection in Asia; however, resistance to such antibiotics was noted (Table 2)[16789101112131415161718]. Antibiotic susceptibility for fluoroquinolones (ciprofloxacin: 19/40, 47.5%; levofloxacin: 13/33, 39.4%) and macrolides (erythromycin: 13/34, 38.2%) was generally low. In addition, Campylobacter species were not susceptible to third generation cephalosporins (3/29, 10.3%). However, they were consistently susceptible to carbapenem agents (imipenem: 9/9, 100%; meropenem: 26/26, 100%).
An optimal treatment regimen of Campylobacter infection is yet to be established. In this study, cefotaxime was administered as an empirical treatment, and this led to a favorable outcome in the patient. Although microbiological breakpoints of the disk susceptibility test for third generation cephalosporins against Campylobacter were not proposed by EUCAST, the National Committee for Clinical Laboratory Standards (NCCLS) guidelines present the breakpoint for cefotaxime as 23mm [19]. Antibiotic susceptibility of C. jejuni which was isolated in our patients, to ceftazidime showed a diameter as 16mm. Thus, third generation cephalosporin were considered to have an intermediate effect in such cases (Table 1). Definite breakpoints of Campylobacter for various antibiotics need to be established using the disk susceptibility test.
The rising antibiotic resistance of the Campylobacter spp. has been an issue. Since the late 1980s, fluoroquinolone resistance has been rising in several Asian and European countries, as well as in the United States. This could be attributed to local antibiotic usage in animal production. In South Korea, the antimicrobial susceptibility of the Campylobacter spp. to fluoroquinolone was found to be 79.5% (2006-2010). It was lower than erythromycin (87.2%) and gentamicin (92.3%), but higher than ampicillin (69.2%) and cephalothin (7.7%) [20]. The epidemiology of Campylobacter antibiotic susceptibility varies depending on the area and time. Therefore, further investigation on the local anti-microbial resistance trend of Campylobacter is required. Antibiotics should be selected carefully because global antibiotic resistance is gradually increasing and inappropriate antibiotic usage could have fatal outcomes.
In conclusion, Campylobacter infection, with or without bacteremia, should be considered if the patient has a fever or gastrointestinal symptoms. Cases of Campylobacter bacteremia in Asia reveal C. fetus to be the main pathogen. Fluoroquinolones and macrolides would be considered as empirical treatment agents based on the local epidemiology of antibiotic resistance. As for the third generation cephalosporins, microbiological breakpoints should be established in the disk diffusion test with respect to clinical outcomes.
Go to :
 XML Download
XML Download