

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Adenovirus (ADV) is one of the most common respiratory pathogens in childhood, and 13-17% of children hospitalized with a viral respiratory tract infection are diagnosed with an ADV infection [123]. Although most cases are self-limiting [34], ADV infection can lead to more severe complications and death. Specific serotypes of the ADV (serotypes 1, 3, 5, 7, 8, 21, and 55), a younger age (less than one year), and immunocompromised hosts have been reported as risk factors for severe ADV infection [567891011].
Recently, multiplex polymerase chain reaction (PCR) tests, which are more sensitive and cost-effective than conventional antigen detection and culture methods, have been used for diagnosing respiratory viral infections [1213]. More cases of multiple respiratory viral infections have been diagnosed using these multiplex PCR tests than were reported before using conventional testing methods [121314]. Consequently, the clinical impact of respiratory viral coinfections, especially coinfection with respiratory syncytial virus (RSV), has been evaluated since the 2000s [15]. In a recently published meta-analysis, respiratory viral coinfections were not reported to result in a significant increase in the clinical severity of respiratory infections compared with single viral infections [15]. However, their clinical effects vary depending on the coinfected viruses and the subjects enrolled in each study. Therefore, while respiratory viral coinfections reportedly manifest as more severe illnesses in some studies [1617], other investigators report a lack of association between viral coinfection and disease severity in ADV infected children [18]. Furthermore, even as ADV infection occurs steadily all year round in Korea, the clinical impact of respiratory viral coinfection on childhood ADV infection has rarely been reported [19]. In addition, previous studies on ADV coinfections included only children younger than 1 or 3 years of age, or children with lower respiratory tract infections [182021]. This retrospective study was performed to investigate the clinical impact of respiratory viral coinfections in Korean children with ADV infection.
Materials and Methods
1. Patients and data collection
The medical records of children (below 20 years of age) admitted to the Department of Pediatrics at Seoul St. Mary’s Hospital, and diagnosed with ADV infection between January 2012 and December 2014, were retrospectively reviewed. Children with immunocompromised status (e.g., underlying hematological malignancy, bone marrow failure syndrome, or an autoimmune disorder requiring immunosuppressant therapy) were excluded. The enrolled children were divided into two groups based on the result of multiplex PCR test for common respiratory viruses. The ADV group included children infected by only ADV, whilst the coinfection group included children concurrently infected with two or more viruses including ADV.
Demographic data included age and sex. Clinical data included birth history, the presence of siblings, the presence of underlying medical conditions, duration of fever and hospitalization, presenting symptoms on admission, final diagnosis on discharge, and severity of the ADV infection. Fever was defined when the tympanic membrane temperature was ≥38.0 ºC. Among presenting symptoms, respiratory symptoms included cough, rhinorrhea, sputum, nasal stuffiness and dyspnea, and gastrointestinal symptoms included vomiting, diarrhea and abdominal pain. Ophthalmologic symptoms included conjunctival injection, ocular pruritus, ocular pain and eye discharges. Neurologic symptoms included dizziness, headache and seizure-like motion, and dermatologic symptoms included various types of skin rashes. The ADV infection was considered severe in cases where oxygen therapy was given; the demand for oxygen increased in a child who had already received oxygen therapy; a child was admitted to the intensive care unit (ICU); or a child died due to the ADV infection. On admission, blood tests were performed to assess total and differential white blood cell counts and platelet counts. In addition, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), aspartate transaminase, and alanine transaminase levels were also assessed at admission. Demographic, clinical, and laboratory parameters were compared between the two children groups. This study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital (Approval No.: KC15RISI0767). Informed consent was waived for this study.
2. Diagnosis of respiratory tract infection
On admission, a nasopharyngeal swab was collected from children complaining of respiratory symptoms or fever without a focus. Samples were sent, as soon as possible, to the Department of Laboratory Medicine where a multiplex PCR test for respiratory viruses was conducted. The commercially available AdvanSure™ RV real-time PCR kit (LG Life Sciences Ltd., Seoul, Korea) was used to detect ADV, influenza A and B viruses, RSV, parainfluenza virus, rhinovirus, coronavirus, human metapneumovirus, and human bocavirus. A positive PCR result for ADV confirmed an ADV infection. If the PCR result was positive for only ADV, the child was assigned to the ADV group, and if the PCR result was positive for two or more viruses including ADV, the child was assigned to the coinfection group.
Upper respiratory tract infection (URTI) included acute pharyngitis, pharyngoconjunctival fever, and acute otitis media, while lower respiratory tract infection (LRTI) included acute bronchiolitis, acute bronchitis, and pneumonia.
3. Statistical analysis
Statistical analyses were performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). Categorical variables between the two study groups were compared using a chi-square test, and continuous variables were compared using a Mann-Whitney test. Factors identified as significantly different between the ADV and coinfection groups in a univariate analysis were assessed for association with coinfection through a multivariate analysis using a binary logistic regression test. A P value of <0.05 was considered as statistically significant.
Results
1. Characteristics of children diagnosed with ADV infection
In total, 105 children were diagnosed with an ADV infection during the study period. The median age at enrollment was 29 months (range: 0-131 months), and 60 (57.1%) children were males. On admission, 104 (99.0%) children complained of fever, and the fever persisted for a median of 5 days (range: 0-13 days) [starting 3 days (range: 0-10 days) before admission and persisting until 2 days (range: 0-5 days) after admission]. Among the local symptoms presented on admission, respiratory symptoms (87 children, 82.9%) were the most frequent, followed by gastrointestinal (24 children, 22.9%) and ophthalmologic (18 children, 17.1%) symptoms. Among gastrointestinal symptoms, diarrhea (17 children, 70.8%) was most frequent, and vomiting (11 children, 45.8%) and abdominal pain (7 children, 29.2%) followed. Febrile seizures occurred in four (3.8%) children. Five children (4.8%) showed fever without localizing signs. URTI and LRTI were diagnosed in 56 (53.3%), and 32 (30.5%) children, respectively. Thirteen (12.4%) children had underlying medical conditions. Eleven (10.5%) children were born prematurely and eight (7.6%) of them also had a previous history of bronchopulmonary dysplasia (BPD); one child had an underlying congenital hypotonia and had experienced recurrent pneumonia since birth; and one child received corrective surgery for esophageal atresia and experienced recurrent respiratory tract infections since the surgery.
Five (4.8%) of the children enrolled in the present study received oxygen therapy, one (1.4%) child in the ADV group and four (12.5%) children in the coinfection group. The child in the ADV group was diagnosed during hospitalization for preterm birth and neonatal respiratory distress syndrome (RDS). He was admitted to the neonatal ICU at birth, received ventilator care and surfactant replacement therapy, and was extubated on hospital day 6. However, fever and apnea developed on hospital day 25, and he received ventilator care again. ADV infection was diagnosed at this time, and he was extubated on hospital day 36. The four children in the coinfection group received oxygen therapy for less than 3 days: two children were born prematurely and had a history of BPD, one child had underlying congenital hypotonia, and the remaining one child was previously healthy.
2. Comparison between ADV and coinfection groups
Thirty-two (30.5%) children were included in the coinfection group (Table 1). Of these, two viruses were simultaneously identified in 28 children (26.7%), and three viruses were simultaneously identified in 4 children (3.8%): ADV, rhinovirus and influenza B virus in one, ADV, rhinovirus and coronavirus in another, and ADV, rhinovirus and human bocavirus in the others. Rhinovirus (n = 15, 41.7%) and RSV (n = 7, 19.4%) were the most commonly coinfected viruses (Table 1).
Table 1
The frequency of respiratory viral coinfections
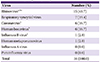
aRhinovirus and coronavirus were concurrently identified in one child.
bRhinovirus and human bocavirus were concurrently identified in two children.
cRhinovirus and influenza B virus were concurrently identified in one child.
![]()
The proportion of children younger than 24 months was significantly higher in the coinfection group compared with the ADV group (P <0.001, Table 2). The children in the coinfection group had a significantly higher tendency for underlying medical conditions (P = 0.020), LRTI (P = 0.011), and need for oxygen therapy (P = 0.029), compared with children in the ADV group (Table 2). However, the duration of fever and hospitalization was not significantly different between the two groups (Table 2). Among laboratory test results, only absolute lymphocyte count (ALC) showed a significant difference between the two study groups (Table 3). The ESR and CRP levels were lower in the coinfection group than in the ADV group; however, this difference was not statistically significant (Table 3). In a multivariate analysis, only the younger age was significantly associated with respiratory viral coinfection (P <0.001, Table 4).
Table 2
Comparison of demographic and clinical characteristics between ADV and coinfection groups

a
P-values for comparison between ADV and coinfection groups.
b
P-values < 0.05 for comparison between ADV group and ADV with rhinovirus coinfection group.
c
P-values < 0.05 for comparison between ADV group and ADV with RSV coinfection group.
ADV, adenoviurs; RSV, respiratory syncytial virus; NA, not available.
![]()
Table 3
Comparison of laboratory test results between ADV and coinfection groups

aESR was tested in 100 children (70 in the adenovirus group, 30 in the coinfection group)
ADV, adenovirus; WBC, white blood cell; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; AMC, absolute monocyte count; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; AST, aspartate transaminase; ALT, alanine transaminase.
![]()
Table 4
Multivariate analysis to determine the factors significantly associated with respiratory viral coinfections

![]()
As rhinovirus and RSV were the most common coinfected viruses, the ADV group was also compared with the ADV and rhinovirus coinfection group and the ADV and RSV coinfection group (Table 2). Children in the ADV and rhinovirus coinfection group tended to be younger and have more underlying medical conditions, and LRTIs compared with those in the ADV group; however, they did not receive more oxygen therapy. Similarly, children in the ADV and RSV coinfection group also tended to be younger, have more underlying medical conditions, and receive more oxygen therapy compared with those in the ADV group; however, the proportion of children with LRTIs was not significantly different between the two coinfection groups.
Discussion
In the present study, clinical and laboratory characteristics of ADV infection in children were investigated, and the clinical impact of respiratory viral coinfection was determined. Respiratory viral coinfection caused more LRTI and a higher need for oxygen therapy than ADV single infection. However, coinfection did not lead to mortality, and the duration of fever and hospitalization was not significantly different between ADV and coinfection groups.
ADV infection in the present study occurred at a median age of 29 months, and in agreement with previous reports, occurred more frequently in males than in females [39192223]. All children except one complained of fever on admission, with fever lasting for a median of 6 days, as is consistent with published reports [34192223]. Respiratory symptoms were most frequent, followed by gastrointestinal symptoms, and this was comparable with previous data [222324]. In the present study, ADV caused more URTIs than LRTIs, even as the current literature provides contradictory evidences, with some reporting a predominance of URTIs [42526], whilst others report a predominance of LRTIs [2324].
Respiratory viral coinfections have been identified in 1.8% - 49.2% of respiratory tract infections in previous studies [1214202728]. The variability in the reported coinfection frequency could be due to the methods of viral detection, the number of detectable viruses, the characteristics of enrolled patients, the frequencies of underlying disorders, the seasons when the studies were performed, and the inclusion or exclusion of URTI [1428]. Most studies reported a higher frequency of respiratory viral coinfection in younger children than in older children and adults [12142728]. This presumably was caused by immature immune systems, the lack of protective immunity arising from prior exposures to viruses, and prolonged excretion of respiratory viruses in younger children compared with older children and adults [142128]. Although respiratory viral coinfection increased the rate and duration of hospitalization [141727], it eventually did not cause a poorer prognosis such as oxygen supplementation and ICU admission, compared with single viral infection [1727]. In a recent meta-analysis, the overall effect of respiratory viral coinfections on the disease severity and prognosis was not significant [15].
In the present study, respiratory viral coinfection was identified in 30.5% of the enrolled children with ADV infection. This coinfection frequency was within the reported range (9.4 - 69.6%) [41922]. Rhinovirus was the most commonly coinfected virus in the present study with RSV being the second, and this was in concurrence with prior published reports [192228].
Previous studies have reported significant association between younger age and coinfection in ADV infection, as is the case with other respiratory viral infections [18192122], and the present study also showed a significant increase in coinfection frequency in children younger than 24 months of age than that in older children. In addition, the increased LRTI cases we report in the coinfection group have been reported previously [1924]. In the present study, we observed a significant association between the presence of underlying medical conditions and coinfection, although this has not been a significant coinfection associated factor in some other previous studies [1822]. Eleven of 13 children with underlying medical conditions in the present study had a preterm birth history, and eight of them had a previous history of BPD. These medical conditions may affect the lower respiratory tract function during infancy and early childhood. Amongst younger age, LRTI, and underlying medical conditions, factors related to coinfection based on a univariate analysis, only the younger age was associated independently with coinfection following a logistic regression test.
Respiratory viral coinfection in ADV infection may cause prolonged hospitalization with or without increase in disease severity, represented by oxygen supplementation and ICU admission [172021]. Some other investigators have, on the other hand, reported no significant effect of coinfection on the duration of hospitalization and disease severity [1822]. In the present study, coinfection caused more LRTIs compared with ADV single infection, and therefore, manifested as more clinically severe and progressive disease than ADV single infection. In addition, oxygen therapy was administered more frequently in the coinfection group, especially in children coinfected with ADV and RSV, than in the ADV group. However, the oxygen supplementation duration in the coinfection group was less than 3 days, and there was no ICU admission and mortality in this group. Furthermore, the duration of hospitalization and fever was not significantly different between the coinfection and ADV groups. This suggested that even as respiratory viral coinfection may contribute to increased disease severity in children with ADV infection, appropriate treatment for such a condition can prevent further disease progression and poor prognosis.
The present study had several limitations, its retrospective nature being the first. We did not identify infecting ADV serotypes in our study, and the severity of ADV infection, as well as frequency of respiratory viral infection, varied according to the causative serotype [891011]. To evaluate the impact of specific ADV serotypes on clinical severity and frequency of coinfections, a multicenter study, involving several geographically-separated hospitals would need to be conducted for a sufficiently long period to capture multiple ADV outbreaks with different causative serotypes. Attending daycare centers may further increase the risk of exposure to a variety of respiratory viruses, and influence the frequency and severity of respiratory viral infections; however, this was not evaluated in the present study. We also could not determine the independent effect of each respiratory virus concurrently identified with ADV infection because of the small group size for each respiratory virus. Finally, the impact of coinfection on the long-term sequelae of ADV infection (e.g., bronchiectasis and bronchiolitis obliterans) could not be assessed [2930].
In conclusion, respiratory viral coinfection in children with ADV infection occurred more frequently in children younger than 24 months of age compared with children aged 24 months or older, and respiratory viral coinfection increased the proportion of LRTI and oxygen therapy requirement. However, appropriate therapy prevented prolonged hospitalization and poor prognosis due to coinfection. Clinicians should thus be more mindful of younger children diagnosed with ADV infection, and be aware of possible coinfections and faster disease progression.
 XML Download
XML Download