

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Aeromonas species, belonging to the genus Aeromonas, are oxidase-producing Gram-negative rods that can grow on MacConkey agar and ferment carbohydrates[1]. These aquatic microorganisms have been associated with a variety of human diseases [1]. Aeromonas species are proliferative and omnipresent in both fresh water and soils [2], and are occasionally isolated from the feces of healthy people [3]. Among 14 known species identified in the genus Aeromonas, many, although not all, are considered to be pathogenic [4]. More than 85% of Aeromonas-implicated clinical diseases are caused by the Aeromonas hydrophila, Aeromonas caviae, and Aeromonas veronii biovar sobria [2]. These infections are acquired in both community and hospital settings, and both immunocompetent and immunocompromised patients are susceptible. Aeromonas species can cause invasive and fatal infections in immunocompromised hosts and have been recognized as a serious threat to human beings [4].
The Aeromonas infection-related disease spectrum in humans has expanded; it now includes acute gastroenteritis, bacteremia, pancreatitis, hepatobiliary-tract infections, soft-tissue infections, indwelling-device-related infections, brain abscesses, meningitis, endocarditis, pleuropulmonary infections, peritonitis, and hemolytic-uremic syndrome [12345678]. The most common underlying conditions known to be associated with Aeromonas bacteremia are malignancy and hepatobiliary diseases [5]. Aeromonas spp. tend to produce at least three ß-lactamases, namely a penicillinase, cephalosporinase, and carbapenemase, which are all chromosome-encoded [6]. Nevertheless, to date, antibiotic resistance has not been a major problem for strains isolated from the environment. In contrast, clinical studies of Aeromonas infections are relatively rare, and the relevant antibiotic susceptibility profile, accordingly, remains vague. Previous studies have attempted to identify risk factors; however, those studies considered only a few risk factors and resistance to a limited number of antimicrobials [278]. Aeromonas bacteremia in patients with cirrhosis or malignancy has been found to be associated with a higher mortality rate than bacteremia caused by other organisms [8]. The present study is the largest retrospective clinical investigation to analyze various data on monomicrobial Aeromonas bacteremia.
The objectives of this study were to elucidate the clinical characteristics of Aeromonas bacteremia and to scrutinize the antimicrobial susceptibility of Aeromonas to optimal therapy. We also aimed to identify risk factors for mortality in patients with Aeromonas bacteremia.
Material and Methods
1. Patients
We retrospectively reviewed the medical records of patients who were diagnosed with Aeromonas bacteremia between January 2000 and December 2013 in multiple centers (Samsung Medical Center [Seoul], Dankook University Hospital [Cheonan], Dong-A University Hospital [Busan], and Jeju University Hospital [Jeju]). Patient records and information were anonymized and de-identified prior to analysis. Institutional review board approval was obtained for retrospective evaluation of the patients (DKUH 2015-01-014).
Aeromonas bacteremia was defined as the presence of an Aeromonas-positive blood culture, with concomitant signs and symptoms of infection. When the patient’s blood culture yielded only one type of pathogen, monomicrobial bacteremia was diagnosed; when more than one type of pathogen was identified, the diagnosis of polymicrobial bacteremia was made. We included only patients with monomicrobial bacteremia in our analysis. Hospital-acquired infections were defined as bacteremic episodes detected at least 72 h after admission in patients who showed no clinical evidence of bacteremia on admission.
Information on age, sex, underlying disease, blood laboratory data, culture results, probable portals of entry, type of antimicrobial agents for treatment, type of medical procedure during treatment, and clinical outcome was collected for each of the patients. Illness severity and comorbidity at the patients’ first presentation with bacteremia to the hospital were graded using the Pitt bacteremia score [59] and Charlson’s weighted comorbidity index [5], respectively. Patients with Aeromonas bacteremia were surveyed for concomitant infection foci; those lacking such foci were classified as having primary bacteremia.
2. Antimicrobial susceptibility test
Aeromonas isolates were obtained by processing of blood culture samples in a BACTEC Model 9240 (BD Diagnostic Instrument Systems, Sparks, MD, USA) or BacT/ALERT 3D (bioMerieux. Inc., Haselwood, MO, USA). Aeromonas was identified by means of a standard identification card. Antibiotic susceptibility testing of the isolates was carried out via an automated system at each hospital. Quality-control protocols and minimum inhibitory concentration breakpoints (MICs) were used in compliance with the standards established by the Clinical and Laboratory Standards Institute [8].
3. Statistical analysis
Statistical analyses were carried out in SPSS 13.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as the mean and standard deviation (SD) or median (range) according to their homogeneity. The categorical variables were compared using the Chi-Square test or Fishers exact test (when necessary). The quantitative variables were compared using the Student–Fisher t test or analysis of variance. The risk factors for infection-related mortality were evaluated by univariate and multivariate logistic regression analyses. Factors with a P-value of 0.2 in the univariate analysis, excepting those considered to be strongly associated with other variables, were entered into the multiple logistic regression analysis. A value of P <0.05 was considered statistically significant.
Results
1. Patient characteristics
Eight-hundred-and-twenty-four cases of Aeromonas bacteremia were enrolled, among which 488 cases of polymicrobial Aeromonas bacteremia were observed. The remaining 336 monomicrobial Aeromonas bacteremia cases were included in this study (Table 1). The major causes of bacteremia were hepatobiliary tract infections (50.6%), followed by peritonitis (18.5%) and primary bacteremia (17.9%). Community-acquired bacteremia was shown in 242 cases (72.0%). The infections usually occurred in patients with solid-organ malignancy (42.3%), hepatic cirrhosis (39.3%), diabetes mellitus (25.6%), or leukemia (7.1%). Concomitant anticancer chemotherapy had been administered in 74 patients (22.0%). The three leading clinical manifestations were fever (38.7%), septic shock (25.6%), and altered consciousness (17.9%). Initial usage of inappropriate antimicrobial agent was noticed in 140 cases. One-hundred-and-sixty-six cases showed antimicrobial-agent combination therapy. The median duration of treatment was 10 days. In 272 cases, antimicrobial-agent initiation within 6 h of symptom manifestations was observed. Fifty patients died of Aeromonas bacteremia.
Table 1
Characteristics of enrolled patients

![]()
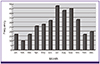
2. Seasonal distribution of Aeromonas bacteremia
A trend toward more frequent occurrence during the warmer seasons (May to October; n = 232; 69.0%) was observed. Most of the community-acquired infections (176 of 242, 72.7%) occurred during these seasons (Fig. 1).
3. Differences in clinical characteristics and antimicrobial susceptibility between species
A. hydrophila was less frequently involved in primary bacteremia and was more frequent in skin and soft-tissue infections and peritonitis (P <0.05) than in infections with other species (Table 2). A. caviae was less prevalent in skin and soft-tissue infections (P = 0.009) and more prevalent in primary bacteremia (P = 0.017) than in infections with other species. Spontaneous bacterial peritonitis (SBP) was more common with A. hydrophila infections (50/62 SBP cases). Pneumonia was more common with Aeromonas salmonicida infection (P <0.001). Hospital-acquired infections were more common among patients with A. caviae and A. salmonicida infections (P <0.001). Underlying diseases differed according to species: A. veronii and A. sorbia infections were more frequent in liver cirrhosis; A. caviae and A. sorbia infections were more frequent in patients with solid-organ cancers; A. salmonicida infections were more common in those with leukemia. Moreover, A. caviae infections occurred more frequently during concurrent chemotherapy (P = 0.004), and A. hydrophila tended to be present in cases of shock (P <0.001). Liver function test results were worse in cases with A. hydrophila infection than in cases with infections involving other species (P = 0.001).
Table 2
Clinical presentation, laboratory findings, and antimicrobial susceptibility in Aeromonas hydrophila, Aeromonas caviae, Aeromonas sobria, Aeromonas veronii, and Aeromonas salmonicida bacteremia

![]()
A. hydrophila accounted for 58.9% of cases; there were 102 cases of A. caviae (30.4%), 20 cases of A. sobria (6.0%), 10 cases of A. veronii (3.0%), and six cases of A. salmonicida (1.7%) infections (Table 2).
All 336 isolates were included in the analysis of antimicrobial susceptibility. More than 90% of cases were susceptible only to ceftazidime, ciprofloxacin, imipenem, gentamicin, and amikacin. Among the five distinct Aeromonas complexes identified, A. hydrophila was more often resistant to antimicrobial agents. The exceptions were the Aeromonas isolates from Jeju University Hospital: these 20 (100%) cases were susceptible to piperacillin, piperacillin/tazobactam, ceftriaxone, ceftazidime, imipenem, ciprofloxacin, tobramycin, gentamicin, and amikacin.
4. Comparison of community-acquired and hospital-acquired Aeromonas bacteremia
No clustered cases of hospital-acquired Aeromonas bacteremia were noted. Individual cases developed within 4–42 days (median: 10 days) after admission. Community-acquired Aeromonas bacteremia differed from hospital-acquired bacteremia in several aspects (Table 3).
Table 3
Comparison of community-acquired vs. nosocomial Aeromonas bacteremia and ceftriaxone-resistant vs. ceftriaxone-susceptible Aeromonas bacteremia

![]()
A total of 242 patients had been diagnosed with community-acquired Aeromonas bacteremia. Univariate analysis revealed statistically significant differences in age, ICU admission, hospital stay, site of infection, underlying diseases (liver cirrhosis, leukemia), concurrent chemotherapy, presence of a central line catheter, blood laboratory results (hemoglobin, prothrombin time [PT], activated partial thromboplastin time [aPTT], aspartate transaminase [AST], bilirubin, and glucose), presence of cardiopulmonary resuscitation, species differences, proportion of initial discordant antimicrobial agent use, initiation of appropriate antimicrobial agent after 6 h, and antimicrobial resistance between community- and hospital-acquired Aeromonas bacteremia. Hepatobiliary infections (P = 0.003) and spontaneous bacterial peritonitis (P = 0.038) were more common in community-acquired bacteremia; primary bacteremia (P = 0.003), pneumonia (P = 0.002), and catheter-related infection (P = 0.000) were more common in hospital-acquired bacteremia. Liver cirrhosis was the common underlying condition in community-acquired bacteremia (P = 0.023), whereas leukemia (P = 0.001) and concurrent chemotherapy (P = 0.002) were the common underlying conditions in hospital-acquired bacteremia. The laboratory findings were more abnormal in cases of hospital-acquired bacteremia (P = 0.009 to 0.045).
5. Antimicrobial therapy
Empirical therapy. Twelve patients died of septic shock with multi-organ failure before appropriate antimicrobial agent treatment could be started. A total of 140 cases were started with inappropriate antibiotics; half of the patients (166) were administered combination therapy, while 56 were placed on aminoglycoside combination therapy. The most common initially administered antimicrobial agents were ceftriaxone and metronidazole (100 cases). Ceftriaxone was the single most common agent in the empirical therapy for Aeromonas bacteremia (61.1%).
Definitive therapy. The therapeutic efficacy of the definitive therapy was evaluated in 310 patients. There were no statistically significant differences in mortality between monotherapy and combination therapy (P >0.050).
Time to the start of antimicrobial agents. There was a statistically significant difference in mortality between the 6 h prior to and after the initiation of appropriate antimicrobial agents (P = 0.049).
6. Ceftriaxone resistance
Among 336 cases of Aeromonas monomicrobial bacteremia, 284 (84.5%) had been caused by ceftriaxone-susceptible (CS) Aeromonas bacteremia and 52 (15.5%) by ceftriaxone-resistant (CR) Aeromonas bacteremia (Table 3). The CS and CR Aeromonas bacteremia groups had similar demographic characteristics. There was a higher rate of mortality in the CR Aeromonas bacteremia group, but this difference was not statistically significant (P = 0.088; Table 3). The CR Aeromonas bacteremia group showed a tendency to disease acquired in a hospital setting (P = 0.002).
7. Outcome analysis for non-survivors
The overall mortality among the 336 patients was 15.0% (50 cases). Death occurred at a median of 10 days post-admission. Twelve patients died within 72 h of their arrival at the hospital. All of the non-survivors had experienced shock. Furthermore, according to univariate analysis, these cases manifested a higher rate of resistance to antimicrobial agents. A number of risk factors for Aeromonas bacteremia-related mortality were found in the multivariate analysis: metastatic cancer, shock, high Pitt bacteremia score, high Charlson’s weighted comorbidity index, high prothrombin time, high serum creatinine level, and initiation of appropriate antimicrobial agents 6 h after manifestation of symptoms (P <0.05 for all variables; Table 4). The predicted Aeromonas monomicrobial bacteremia mortality rate was found to be closely related to the known Pitt bacteremia score.
Table 4
Risk factors for fatality of Aeromonas bacteremia

![]()
Predicted mortality rate (%) = (Pitt bacteremia score × 0.084 + 0.005) × 100
Discussion
Our study included a large number of cases of monomicrobial Aeromonas bacteremia, with full laboratory and medical records; these were amenable to analysis and could provide useful information for better clinical practice.
The three major clinical categories of Aeromonas infection are hepatobiliary tract infection, peritonitis, and primary bacteremia. These have been identified in more than 80% of reported Aeromonas infections. An earlier study found that the most common underlying conditions associated with Aeromonas septicemia were malignancy (21–50%) and hepatobiliary diseases (15–54%) [247121314], although healthy patients were also shown to be susceptible to Aeromonas infection. Likewise, underlying illness with malignancy, hepatobiliary diseases, and diabetes mellitus were frequently encountered in Aeromonas bacteremia in this study. As many as 25.6% of patients in the present study had diabetes mellitus, which was a significantly higher rate than that previously reported 11% [5]. Our data suggested that individuals presenting with Aeromonas bacteremia should be evaluated for the possibility of underlying malignancy, hepatobiliary diseases, or diabetes mellitus.
Previous reports have shown that patients with Aeromonas bacteremia could be treated with one of the broad-spectrum β-lactam agents, such as third-generation cephalosporins, aztreonam, and imipenem, or with fluoroquinolone alone [257]. However, antimicrobial resistance to extended-spectrum cephalosporins (such as cefotaxime) in clinical Aeromonas isolates has been noted [124567111214151617]. Indeed, fluoroquinolone resistance is increasing, as evidenced by the ciprofloxacin-resistance rate of 14% that was previously reported [2]. In the current study, the rates of resistance to ceftriaxone, ciprofloxacin, and imipenem were 15.5, 10.1, and 9.8%, respectively. It has been shown that, for carbapenemase-producing Aeromonas strains, the MICs of imipenem were above 8 mg/L [6]. However, the clinical effect of the inducible carbapenemases in clinical Aeromonas species has not been clearly delineated as yet [26]. One case study reported an imipenem-resistant A. veronii clinical isolate, recovered from a patient with cholangitis; this case also did not show any clinically significant carbapenem-resistance in Aeromonas species [1819]. A history of carbapenem use was associated with mortality in the present univariate analysis. This suggests that previous carbapenem use can induce resistance and thereby lead to a poor clinical outcome.
Based on the resistance rates found in our data, amikacin, gentamicin, ceftazidime, imipenem, and ciprofloxacin are reasonable antimicrobial therapy choices for treatment of Aeromonas infections. Ceftriaxone is the usual empirical treatment of choice for patients with hepatobiliary infections. Ceftriaxone was started as the initial treatment in most cases of suspected gastrointestinal or hepatobiliary infection identified in the present study. The high resistance patterns led to 41.7% of patients being treated with inappropriate empirical antimicrobial therapy. Additionally, ceftriaxone-resistant Aeromonas bacteremia groups showed severe clinical manifestations and laboratory findings. The only exceptions were the Aeromonas isolates from Jeju University Hospital, all of which (n = 20) were susceptible to piperacillin, piperacillin/tazobactam, ceftriaxone, ceftazidime, imipenem, ciprofloxacin, tobramycin, gentamicin, and amikacin. Thus, geographic differences may affect resistance patterns. Recommendations for combination therapy in Aeromonas bacteremia have come from studies of a small number of cases with both polymicrobial and monomicrobial bacteremia [2021]. In contrast, in the current study, there was no significant difference in the clinical outcomes of patients definitively treated with either monotherapy or combination therapy. However, we cannot recommend either monotherapy or combination therapy for treatment of Aeromonas bacteremia at this point, because the proportion of inappropriate initial therapy was high in our experience. Given the lack of available therapeutic options for Aeromonas bacteremia, well-controlled clinical trials of combinations of existing antibiotics are urgently needed.
A. caviae is the most frequent pathogen causing Aeromonas bacteremia in Japan [1922], whereas A. hydrophila, followed by A. veronii biovar sobria, is the most common Aeromonas species causing bacteremia in Taiwan [23]. In our study, A. hydrophila was the most common Aeromonas species causing bacteremia, followed by A. caviae, which is interesting, as Korea is geographically located between China and Japan. Therefore, additional epidemiological studies are required in order to establish the bacteriology of different types of Aeromonas infections in different regions. Isolates need to be collected, and the links between genetic factors and geographic areas should be analyzed. This is relevant, as in this study, A. hydrophila showed higher antimicrobial resistance and resulted in greater clinical severity than did the other Aeromonas spp. (P <0.05).
The mortality rates among patients with Aeromonas bacteremia range from 28 to 63% in the literature [1247182425]. However, our study showed a significantly lower mortality rate (14.9%). In our cases, patients with skin and soft-tissue infection had worse clinical outcomes than did those with other secondary bacteremia; this finding was statistically significant only in univariate analysis. Bacterial peritonitis has been associated with an approximate 15% mortality rate, and necrotizing fasciitis with a higher mortality rate of 50% (one death in two patients). In our study, the number of patients with necrotizing fasciitis was 14. We postulated that the lower mortality rate in our study was associated with a low prevalence of soft-tissue infection as well as a relatively low rate of liver cirrhosis [7]. Inappropriate therapy has been regarded as a prognostic factor in patient outcomes [26], and was correlated with mortality in this study.
The main limitation of this study was its retrospective design. As such, specific information on the antibiotic types (cefepime and aztreonam) used was missing from the medical records. Furthermore, our study was conducted at four tertiary hospitals and examined data spanning 14 years. During that time, medical and microbiological environments changed, and thus our results cannot be generalized to all other hospitals.
In conclusion, patients with Aeromonas bacteraemia can be treated with carbapenem, ceftazidime, or fluoroquinolone. Although Aeromonas species showed a higher resistance rate to ceftriaxone, Aeromonas bacteremia was correlated with a relatively low mortality rate compared with previous studies. All of the non-survivors experienced shock. Ceftriaxone-based metronidazole combination treatment might not be recommendable as an initial empirical therapy, in particular due to the high antimicrobial resistance rates to various agents in septic-shock patients. In patients with septic shock, carbapenem-based aminoglycoside combination treatment may also not be considered as an initial empirical therapy, due to the high antimicrobial-resistance rates to various agents present in septic shock. Considering the risk factors for mortality, adequate antibiotics should be given early, especially to patients with shock and impaired renal function. In order to make recommendations for definitive therapy based on available susceptibility results, further studies with larger numbers of cases and supportive experiment, such as DNA sequencing, are warranted.
 XML Download
XML Download