

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Streptococcus pneumoniae, the pneumococcus, is an important human pathogen that causes serious diseases such as meningitis and bacteremia (infection of normally sterile sites, termed invasive pneumococcal disease or IPD), as well as pneumonia. Pneumococcus is also a common etiologic agent in milder diseases such as sinusitis and otitis media. In 2005, the World Health Organization (WHO) estimated that 1.5 million deaths each year are due to pneumococcal diseases [1]. In 2008, the WHO also estimated that about 0.5 million deaths of 8.8 million total global annual deaths among children <5 years of age were caused by pneumococcal infections [2]. Among elderly patients, the overall case fatality rate for pneumococcal bacteremia is up to 40% [3]. Deaths from pneumococcal bacteremia tend to occur quickly, often within the first week of hospitalization, even in the context of appropriate antibiotic therapy [4]. Therefore, pneumococcal vaccination is an important strategy for the prevention of pneumococcal infection. To this end, many national immunization programs (NIPs), which are government-based programs focused on reducing rates of vaccine-preventable diseases, now include pneumococcal vaccines. The pneumococcal conjugate vaccine (PCV) has been developed to overcome the limitations of the pneumococcal polysaccharide vaccine (PPV), which has poor immunogenicity in infants younger than 2 years of age [5]. Since the initial United States (US) approval of PCV7 in 2000, pneumococcal conjugate vaccines have been adopted into routine infant immunization programs in many countries [6], resulting in a significant reduction in the incidence of IPD among children [78]. In addition to poor immunogenicity among infants, there is also evidence to suggest reduced immunogenicity of PPV among elderly adults and adults with certain immune compromising conditions [9]. Unlike polysaccharide vaccines, such as PPV, which result in antibody production without immune memory, conjugate vaccines such as PCV result in memory B cell production (T-cell-dependent response) that produce a more sustained effect [910]. In accordance with this information, some NIPs now include recommendations for administration of PCV to elderly adults and adults with immune compromising conditions [11]. Reduction in disease in vaccinated individuals is referred to as the “direct” effect of a given vaccine. However, in addition to the direct effect of PCV on reducing pneumococcal disease in the vaccinated population, there has been a concordant decline in the incidence of IPD among adults who did not receive the vaccine following the introduction of PCVs into NIPs for young children [121314]. Reduction in disease within the non-vaccinated population is referred to as the “indirect”, or “herd” effect. In this review, we describe the indirect effect of PCV in pediatric NIPs on adult pneumococcal diseases, specifically how pneumococcal vaccines in NIPs for young children can decrease the incidence of adult pneumococcal disease.
Pneumococcal Vaccines
PCV7 (Prevnar; Pfizer) was introduced in 2000, and included coverage for serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F [15]. PCV10 (Synflorix; GlaxoSmithKline) was licensed in 2008 and included coverage for serotypes 1, 5, and 7F in addition to those covered by PCV7. PCV13 (Prevnar13; Pfizer), licensed in 2009, expanded coverage to include serotypes 3, 6A, and 19A in addition to those covered by PCV10 [15]. PPV23 (PNEUMOVAX23; Merck) includes coverage for 12 serotypes common to PCV13 (1, 3, 4, 5, 6B, 7F, 9V, 14, 18C, 19F, 19A, and 23F) as well as 11 additional serotypes (2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F, and 33F) [15]. In the future, PCVs may include coverage for up to 20 different serotypes [16].
The WHO places estimates of global coverage for pneumococcal vaccines (PPV and PCV) at 37%, with implementation in 129 countries as of the end of 2015 [17]. As of September 2016, 132 countries (68%) have introduced PCV into their routine infant immunization programs, and 6 additional countries (3.1%) plan to introduce PCV into NIPs in 2016 (Fig. 1) [18]. However, since their introduction, PCVs have been licensed and available for optional use in many countries without formal inclusion in NIPs. In Korea, PCV7 was made available as an optional vaccine in 2003 [19], and a NIP for children with PCV10 or PCV13 was implemented in 2014 [17]. The Korea National Immunization Survey found that for children born in 2009, the rate of PCV administration prior to inclusion in the NIP was about 70%. However, PCV administration varied according to region, with a rate of 71.3% in urban areas as compared to 56.8% in rural areas [20]. Notably, 2014 Korean guidelines also recommend administration of either PPV23 or PCV13 to adults ≥65 years old [21].
Figure 1
Countries with Pneumococcal Conjugate vaccine (PCV) in the national immunization program and planned introductions in 2016, adapted to include dates of introduction for PCV for selected countries, organized by WHO region
World Health Organization. Immunization, Vaccines, and Biologicals-Data, statistics and graphics. Updated 01 December 2016. Available at
http://www.who.int/immunization/monitoring_surveillance/data/en
Accessed 7 December 2016.
*Includes partial introduction

Pneumococcal Pathogenesis
Understanding mechanisms for the indirect effect of pediatric vaccines on the unvaccinated adult population depends first upon understanding the mechanisms for carriage and transmission of S. pneumoniae within a population as a whole. Pneumococcus is a commensal flora of the nasopharynx, and humans are its only natural host. Thus, nasopharyngeal carriage and horizontal transmission within human populations represent the sole means for acquisition and spread of pneumococcal disease. As a result, pneumococcal colonization is an essential prerequisite for development of pneumococcal disease [222324]. Most pneumococci are characterized by a polysaccharide capsule, which is the primary determinant of virulence and invasiveness [25262728]. Additionally, the polysaccharide capsule is the basis for classification by serotypes and has been a focus for vaccine development [225262728]. Pneumococcal colonization occurs early in infancy and is most prevalent among young children, with a markedly lower rate of colonization in adults. Pre-PCV data from a large cohort of healthy Dutch children demonstrated that peak incidence of colonization was 55% at age 3, which declined to 8% after age 10 [29]. While the rates of pneumococcal carriage vary primarily by age, they may also be influenced by multiple additional factors, such as baseline serotype-specific prevalence, genetics, socioeconomic status, and demographic variables [2930]. Specifically, crowding and close contact among children (e.g. between siblings and in day care centers) have been identified as significantly affecting transmission [2931]. Consequently, rates of pneumococcal colonization vary widely across different populations. For these reasons, it is important to consider these factors and to conduct population-specific surveillance data in order to predict or evaluate the effects of a vaccine. Prior to the introduction of PCV into the NIP in Korea, the prevalence of pneumococcal carriage was 34% among children aged less than 5 years [32], and 9.6% among those aged 5 to 18 years [19].
Pneumococcal colonization is believed to represent the most important source of horizontal spreading within a community [3031]. Adults acquire nasopharyngeal colonization (and subsequently pneumococcal disease) via contact with children. In older adults, IPD exhibited distinct winter seasonality, especially surrounding winter holidays (Christmas and New Year’s) [3334]. Epidemiologic data also indicates a disproportionate effect of spikes in pediatric serotypes among older adults, particularly older women. Such data suggests the possibility of seasonal increases in transmission related to family contact between elderly adults and young children [34]. Adults with community-acquired pneumonia (CAP) who had regular contact with PCV7-vaccinated children were less likely to have CAP caused by the serotypes covered by the PCV7 vaccine than those with regular contact with unvaccinated children [35]. This can be explained by acquisition of S. pneumoniae from children colonized with similar pneumococcal serotypes via horizontal transmission. These mechanisms for pneumococcal carriage and transmission among children are therefore associated with changes in the burden of adult pneumococcal diseases.
Effects of Vaccination on Pneumococcal Carriage
PCVs have been associated with changes in carriage rates of vaccine type (VT) and non-VT serotypes. In a randomized trial of PCV administration to toddlers attending day care centers, the rate of carriage of VT S. pneumoniae was reduced in the vaccinated group, although that of non-VT was higher than in the control group [36]. Increases in the rate of non-VT carriage or disease after implementation of a vaccine, a phenomenon known as serotype replacement, is of significant concern with any NIP, including pneumococcal vaccines, and warrants careful consideration and surveillance.
In addition to the direct effects on carriage rates in vaccinated children, indirect effects of PCV on carriage rates in non-vaccinated adults have also been observed. The prevalence of VT carriage was lower in adults living with PCV7-vaccinated children than that in adults living with unvaccinated children [37]. In several community-based studies, reductions in the rate of carriage of VT were observed in unvaccinated children and adults after mass pediatric vaccination with PCV7 [3839] or PCV10 [40]. PCV13 also led to a reduction of nasopharyngeal pneumococcal carriage of the serotypes it uniquely covers in vaccinated children [41]. A Massachusetts-based study in the US noted a 50% decline in PCV13 serotype colonization among unvaccinated children at a time when overall vaccine coverage was 75% [42]. This finding suggests that implementation of a NIP could result in a coverage rate sufficiently high to induce an indirect effect.
To summarize the proposed mechanism by which NIP for young children can decrease the incidence of adult pneumococcal disease, PCV first leads to a reduction in VT colonization via a direct effect on vaccinated individuals [3641]. In turn, unvaccinated children and adults experience less exposure to VT serotypes [37], resulting in a reduction in VT-IPD among unvaccinated adults [43].
Effects of Vaccination on Pneumococcal Diseases
1. IPD
Trends in surveillance data from around the world indicate a strong direct effect of PCV in reducing rates of VT-IPD in vaccinated children. Data from Active Bacterial Core Surveillance (ABCs) of the Centers for Disease Control and Prevention (CDC) in the US indicate a rapid decrease in the incidence of VT-IPD among US children younger than 2 years of age, from 156.1 cases per 100,000 persons in 1998 and 1999 to 33.6 per 100,000 in 2001, reflecting a 78% decrease in the rate of VT-IPD in this population [8]. There was a steady and continued decline in rates of VT-IPD in children over the seven years following the introduction of PCV7 [4445], as well as a significant decrease in overall IPD [4546]. Surveillance data from Calgary, Alberta suggested near-total elimination of VT-IPD caused by PCV7 serotypes, with no documented cases from 2007-2013 within the study population [47]. Danish data also supports this conclusion regarding PCV7 VT-IPD [48]. After replacement of PCV7 with PCV13, the incidence of IPD caused by serotypes unique to PCV13 also decreased significantly in children less than 2 years of age [474849505152].
Epidemiologic data also supports the presence of an indirect effect of PCV on reducing rates of VT-IPD among unvaccinated adults. In adults older than 65 years of age, the pre- and post-PCV7 incidence of IPD caused by PCV7 serotypes (in cases per 100,000 persons) were respectively 33.6 and 11.9 in the US [12], 22.1 and 4.8 in Canada (ages 65-84) [13], 27.1 and 14.0 in Denmark [48], and 18.2 and 3.4 in England and Wales [53]. The pre- and post-PCV7 incidences of overall IPD in these populations were 60.1 cases per 100,000 persons and 41.7 cases per 100,000 persons in the US [12], 36.2 and 23.9 in Canada [13], 65.5 and 60.0 in Denmark [48], and 34.8 and 28.2 in England and Wales [53], respectively. The rate of IPD caused by PCV7 serotypes in the unvaccinated population decreased by 64% [12] to 92% [45] after introduction of PCV7. From surveillance data during the 2.5 to 4 years after replacement of PCV7 with PCV13, the rate of IPD in adults older than 65 years of age caused by the additional serotypes included in PCV13 decreased by 18% in Canada [48], 58% in the US [51], 64% in England and Wales [52] and 53% in Israel [54].
While certain PCV7 serotypes were nearly eliminated, serotypes 19A, 3, and 7F (which were among the six additional serotypes included in PCV13) remained the major serotypes responsible for IPD among all adults in a Calgary, Alberta-based Canadian surveillance program [4755]. These findings may be a result of insufficient time after PCV13 introduction to observe an indirect effect in the adult population. A pooled analysis of surveillance data from multiple countries showed that significant reductions in overall IPD among adults were not observed until 7 years after PCV7 introduction, along with a more gradual reduction in rates of VT-IPD than that observed in children [44]. Furthermore, there is some data to suggest reduced efficacy in protection against IPD for some of the additional 6 serotypes unique to PCV13, especially serotype 3 [515253]. Surveillance data from Utah, one of the states in U.S., indicated a nonsignificant decline in serotype 3 IPD following PCV13 implementation [49]; post-licensure data for PCV13 in a Public Health England study indicated lower serotype 3 IgG response than predicted [4956]. In Portugal, serotype 3 remained the most common cause of adult IPD, in contrast to reductions in other PCV13 serotypes, which were attributed to indirect protection [57]. In spite of these findings, fluctuations in serotype-specific rates of disease and low baseline incidence of serotype 3 disease in certain areas may complicate evaluation of vaccine effectiveness [51], and ongoing investigation across multiple regions is indicated.
The issue of serotype replacement in older adults has also emerged after introduction of PCV7 and PCV13. After PCV7 introduction, the incidence of IPD caused by non-VT serotypes in adults ≥65 years old increased from 14.1 cases per 100,000 persons to 18.8 cases per 100,000 persons in Canada (ages 65-84) [13], 18.3 to 22.5 in the US [45], and 16.6 to 24.8 in England and Wales [53]. After PCV7/13 introduction, non-VT IPD increased nonsignificantly from 3.0 to 4.1 in Canada across all age groups [47], and especially among adults ≥65 years old, from 19.7 to 29.4 in Denmark [48] and 12.7 to 16.3 in England and Wales [52]. Despite the increase in non-VT serotypes following introduction of PCV7/PCV13, the overall incidence of IPD across all ages has decreased by 25-45% in the US [1245], 37% in Canada [1347], 20% in Oxfordshire, England [50], and 32%-35% in England and Wales as a whole [5253]. Surveillance data from the US indicates that the greatest reduction in the rate of overall IPD was observed in adults ≥65 years old [12]. While serotype replacement has certainly occurred and must be monitored over time, the reduction in overall IPD suggests a net-beneficial effect of PCV.
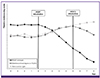
In summary, the rates of VT-IPD and overall IPD in the unvaccinated population, especially adults above 65 years of age (indirect effect), as well as in the vaccinated population (direct effect), decreased after implementation of PCV in national immunization plans for children, although non-VT IPD increased slightly (Fig. 2). The indirect effect after childhood PCV immunization, the decrease in VT-IPD and overall IPD, and the increase in non-VT IPD could be influenced by pre-PCV incidence of IPD, and the length of time after PCV introduction.
2. Pneumococcal pneumonia
There are few studies concerning the indirect effect of childhood immunization on adult pneumococcal pneumonia without bacteremia, since the microbiologic diagnosis of pneumonia without bacteremia is difficult. Both lower respiratory tract culture and rapid urine antigen testing (UAT), which represent the most widely utilized diagnostic techniques for etiologic diagnosis of pneumococcal pneumonia, are limited by a lack of sensitivity. A systematic review and meta-analysis that included studies utilizing these diagnostic methods estimated that 27.3% of community-acquired pneumonia was attributable to S. pneumoniae [58]. However, as 75% of all pneumococcal pneumonia in adults is non-bacteremic [58], the indirect effect may be underestimated based on bacteremic pneumococcal pneumonia classified as IPD. The relatively recent development of multiplexed serotype-specific urine assays for the detection of pneumococcal antigen have allowed for the estimation of serotype prevalence as well as vaccine effects on CAP [59].
These assays have provided evidence to support the concept of indirect protection for adult CAP as a result of childhood vaccines. Implementing one such assay, Pletz et al. found that in adult CAP, the proportion of PCV7 serotypes decreased from 30.6% in 2002-2006 to 13.3% in 2007-2011 in Germany, following implementation of PCV7 in the NIP for children in 2007 [59]. In a prospective cohort study beginning eight years after PCV7 introduction and 3 years after PCV13 introduction in the UK, the incidence of adult CAP caused by PCV7 serotypes and additional PCV13 serotypes declined by 88% and 30% respectively, also as detected by a serotype-specific urine assay [60]. This data suggests that trends in indirect effects of mass childhood PCV immunization on adults with CAP correspond with those noted for IPD.
Recent studies have also sought to examine the direct effects of administering PCV to elderly adults, and have led to growing inclusion of PCV in adult NIPs. The Community-Acquired Pneumonia immunization Trial in Adults (CAPiTA) was a large, randomized, placebo-controlled trial to evaluate the efficacy of PCV13 in preventing pneumonia due to PCV13 serotypes in Dutch adults 65 years of age and older, also using a multiplexed serotype-specific urine assay. Study enrollment began 2 years after implementation of PCV7 into the pediatric national immunization program in the Netherlands, and PCV10 replaced PCV7 during the study. The trial demonstrated efficacy of PCV13 for VT-CAP, however it failed to demonstrate efficacy when non-VT serotypes were included [61].
To examine the indirect effects of PCV on CAP in elderly adults, a post hoc analysis was conducted on the 270 cases of non-bacteremic pneumococcal CAP from 42,256 subjects in the placebo (i.e. non-vaccinated) arm of the CAPiTA study. This analysis found that PCV7 serotypes decreased from 28% to 7%. There was no reduction in the additional PCV10 and PCV13 serotypes, and non-PCV13 serotypes increased from 30% to 37% [62]. While these findings support concordant trends in indirect protection from both PCV7 CAP and IPD among the elderly adult population, they also suggest a similar trend in serotype replacement for pneumococcal CAP and IPD. Likewise, the lack of reduction in PCV10 and PCV13 serotypes in this population presents similar possibilities as data for IPD. Since the study period included data through 2013 (two years after switch to PCV10 in the NIP), the lack of reduction among the expanded serotypes raises the possibility of reduced vaccine efficacy for PCV10 or PCV13 serotypes, or that there was insufficient time to observe an indirect effect. Novel diagnostic techniques offer new opportunities for surveillance of pneumococcal CAP to more thoroughly assess the indirect effects of PCV.
Perspective after introduction of pneumococcal vaccine NIP in Korea
In 2014, the US Advisory Committee on Immunization Practices (ACIP) recommended that PCV13 should be administered to all adults 65 years of age or older, given in series with PPV23. This recommendation was, in large part, based on the result of the CAPiTA study [11]. In 2018, ACIP plans to reevaluate recommendations for routine PCV13 use among adults 65 years of age or older to incorporate available findings regarding the indirect effect of PCV13 [11]. Prior to the introduction of PCV13, the serotypes contained in PCV10, PCV13, and PPV23 accounted for 39.8%, 67.3%, and 73.4% of pneumococcal infections, respectively, among Korean adults 19 years of age or older [63]. Based on this information, the Korean Society of Infectious Diseases (KSID) recommended that either PCV13 or PPV23, but not both, should be administered to healthy adults 65 years of age or older [21].
Following implementation of a PCV-containing NIP for Korean children in 2014, serotypes causing pneumococcal diseases may be redistributed as serotype replacement occurs. Following implementation of PCVs, studies of surveillance data have noted an increase in disease caused by serotypes found solely in PPV23 [57]. This could effectively broaden the coverage range of PPV23 for adults, which would provide coverage for 11 additional non-PCV13 serotypes. A systematic review and meta-analysis suggested that the vaccine effectiveness of PPV23 in preventing IPD and all-cause CAP was similar to the estimates for PCV13, as reported in the CAPiTA trial [64]. Therefore, the role of PPV23 in adults may be more important in the context of pediatric PCV NIP. However, this theoretical benefit must be weighed against the potential for a reduced direct effect due to the relatively lower immunogenicity of PPV in certain adult populations. As post-PCV trends in indirect protection and serotype replacement are dependent on numerous factors that are specific to a given population, ongoing surveillance is necessary to evaluate the overall effects of PCV and to determine the ideal strategy for pneumococcal vaccine administration in Korean adults.
 XML Download
XML Download