

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The emergence and spread of antibiotic-resistant bacteria is of great concern to physicians because they can cause serious and even fatal infections in hospitalized patients. The circulation of multidrug resistant (MDR) non-lactose-fermenting gram-negative pathogens in hospital settings is widespread and increasing in many countries, representing a serious global health threat [1]. Among them, Acinetobacter baumannii, a ubiquitous, strictly aerobic, non-fermentative coccobacillus, has emerged as a major cause of nosocomial infections, especially in intensive care units (ICUs) [2]. A. baumannii is a frequent cause of nosocomial pneumonias, mainly ventilator-associated, and of bloodstream infections in immunocompromised and debilitated patients with serious underlying diseases. It has also been implicated in complicated skin and soft tissue infections, nosocomial cases of endocarditis, abdominal and urinary tract infections, and central nervous system infections in neurosurgical patients.
A. baumannii is intrinsically resistant to many antibiotics and disinfectants because of the low permeability of its outer cell membrane and the constitutive expression of certain efflux pumps, and it can accumulate components of resistance mechanisms encoded on plasmids, transposons, and integrons in hospital settings associated with high antibiotic consumption [23]. Further, A. baumannii has the ability to survive for extended periods of time on inanimate surfaces, such as hospital equipment [4].
Over the last 20 years, a tremendous rise in the rates of multidrug resistance to most antimicrobial agents that are active against A. baumannii has been noted worldwide, to the point that carbapenems are no longer considered salvage therapy [5]. In several studies, infection with MDR A. baumannii has been associated with increased mortality [678]. Thus, continuous surveillance of antimicrobial resistance of A. baumannii is extremely important for the selection of appropriate empirical therapy for seriously ill hospitalized patients because it can increase their chances of survival.
The current study evaluated the rates of antibiotic resistance and changes in resistance of A. baumannii isolated from hospitalized patients over 5 consecutive years (2010–2014), in relation to patient setting in a tertiary Greek hospital.
Materials and Methods
We retrospectively analyzed all clinical A. baumannii strains that were collected and processed by the microbiological laboratory in our hospital from January 2010 to December 2014. The study hospital is a 700-bed, tertiary care, general hospital serving a population of 683,000 people (2011 national census). Blood, respiratory tract specimens, urine, pus from wounds, and other biological specimens collected from patients admitted to any unit of the hospital were eligible for inclusion. Only the first isolate per patient was included in the study. This study was approved by the ethics committee of the hospital, with approval to report microbiological and laboratory data as part of routine medical care.
Bacterial species were identified by standard biochemical methods and the Vitek 2 automated system (bioMérieux SA, Marcy L’ Etoile, France). Vitek 2 was also used for antimicrobial susceptibility testing. The 18 antimicrobials tested were: ampicillin/sulbactam, ticarcillin, ticarcillin/clavulanic acid, piperacillin, piperacillin/tazobactam, cefotaxime, ceftazidime, cefepime, imipenem, meropenem, gentamicin, amikacin, tobramycin, ciprofloxacin, tetracycline, tigecycline, trimethoprim/sulfamethoxazole, and colistin. In addition, the minimum inhibitory concentrations (MICs) of amikacin, tigecycline, and colistin were determined by the E-test method (bioMérieux SA, Marcy L’ Etoile, France), following the manufacturer's recommendations. All tests were performed in duplicate. The Clinical and Laboratory Standards Institute (CLSI) MIC breakpoints were used to interpret the results of all antimicrobial agents except for tigecycline, for which the Food and Drug Administration (FDA) breakpoints were applied [910]. Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as quality control strains.
Multidrug resistance was defined as resistance to ≥3 classes of antimicrobial agents.
Resistance of A. baumannii clinical isolates to individual antimicrobial agents is presented in absolute numbers and percentages, and was analyzed by year, and hospital unit origin (ICU vs. surgical wards vs. medical wards). Rates were compared using a χ2 test for a row-by column contingency table with appropriate degrees of freedom. P values <0.05 were considered statistically significant. All statistical analyses were performed with Graphpad Prism version 4 (GraphPad Software Inc, La Jolla, CA, USA).
Results
Overall, 914 clinical isolates of A. baumannii were recovered over the 5-year study period. These were recovered from the ICU (n = 493), and medical (n = 252) and surgical (n = 169) wards. The vast majority of strains originated from adult patients (n = 887), with the remaining (n = 27), originated mainly in the pediatric ICU. As shown in Table 1, the highest number (n = 211) of strains was isolated in 2010, and the lowest (n = 148) in 2013. Table 1 shows the antibiotic susceptibility (absolute numbers, rates, and statistical significance of differences) of isolates by year of collection. The most effective antimicrobial agents in order of frequency were: colistin, amikacin, trimethoprim/sulfamethoxazole, tigecycline, and tobramycin. However, with the exception of colistin, no antibiotic was associated with a susceptibility rate >40% for the entire study period.
Table 1
Antibiotic susceptibility (absolute numbers, rates, χ2 statistical comparison) of 914 Acinetobacter baumannii clinical isolates by year
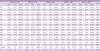
S, susceptible; I, intermediate; R, resistant; SAM, ampicillin-sulbactam; TIC, ticarcillin; TIM, ticarcillin-clavulanic acid; PIP, piperacillin; TZP, piperacillin-tazobactam; CTX, cefotaxime; CAZ, ceftazidime; FEP, cefepime; IPM, imipenem; MEM, meropenem; GEN, gentamicin; AMK, amikacin; TOB, tobramycin; CIP, ciprofloxacin; TET, tetracycline; TGC, tigecycline; TMP/SMX, trimethoprim-sulfamethoxazole; CST, colistin.
![]()
As shown, with the exception of ampicillin/sulbactam, ticarcillin, piperacillin, piperacillin/tazobactam, cefotaxime, ceftazidime, cefepime, and ciprofloxacin, highly statistically significant changes in resistance by year were noted against the remaining 10 antibiotics tested. The overall rate of resistance (fully resistant and intermediate susceptible) to ampicillin/sulbactam was 92.45%; to ticarcillin, 94.42%; to piperacillin, 96.06%; to piperacillin/tazobactam, 93.33%; to cefotaxime, 97.26%; to ceftazidime, 94.64%; to cefepime, 94.09%; and to ciprofloxacin, 93.33%. For the remaining antibiotics, for which significant changes in resistance were noted over time, the overall rates of resistance were the following: ticarcillin/clavulanic acid, 93.44%; imipenem, 88.95%; meropenem, 86.98%; gentamicin, 83.59%; amikacin, 60.28%; tobramycin, 69.69%; tetracycline, 93.11%; tigecycline, 64.99%; trimethoprim/sulfamethoxazole, 63.57%; and colistin, 2.95%. Susceptibility to tigecycline progressively decreased over the study period, with intermediate susceptibility isolates predominating in the early years (2010–2011) and resistant isolates in 2012–2014. Although colistin resistance was low, 20 of 27 (74%) resistant isolates were recovered in the two most recent study years.
Table 2 shows the antibiotic susceptibility (absolute numbers, rates, and statistical significance of differences) by specimen origin (ICU vs. surgical wards vs. medical wards) for all clinical isolates. As shown, for 14 of the antimicrobials tested, statistically significant differences in resistance were noted by hospital unit origin. For all antibiotics, except colistin, for which significant differences by hospital unit origin were noted, ICU strains were more resistant, followed by surgical wards and then by medical wards strains. Only 1 of 27 isolates resistant to colistin originated from a medical ward, with the vast majority coming from the ICU (n = 17) and surgical wards (n = 9). Colistin strains from surgical wards showed higher rates of resistance than ICU strains. No significant differences in antibiotic susceptibility by hospital unit origin were noted for amikacin, tobramycin, tigecycline, or trimethoprim/sulfamethoxazole.
Table 2
Antibiotic susceptibility (absolute numbers, rates, χ2 statistical comparison) of 914 Acinetobacter baumannii clinical isolates by hospital unit origin
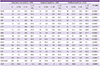
S, susceptible; I, intermediate; R, resistant; SAM, ampicillin-sulbactam; TIC, ticarcillin; TIM, ticarcillin-clavulanic acid; PIP, piperacillin; TZP, piperacillin-tazobactam; CTX, cefotaxime; CAZ, ceftazidime; FEP, cefepime; IPM, imipenem; MEM, meropenem; GEN, gentamicin; AMK, amikacin; TOB, tobramycin; CIP, ciprofloxacin; TET, tetracycline; TGC, tigecycline; TMP/SMX, trimethoprim-sulfamethoxazole; CST, colistin.
![]()
Table 3 shows the resistance phenotypes by year of isolates tested over the entire 5-year study period (2010–2014). As shown, only 4.9% of these isolates were fully susceptible to the tested antimicrobials, whereas 92.89% of them were MDR. The five most common resistance phenotypes represented 84.25% of all MDR isolates.
Table 3
Resistance phenotypes of Acinetobacter baumannii isolates by year to antimicrobials tested over the entire 5-year study period (2010–2014)

CST, colistin; CEF, cephalosporins; SAM, ampicillin-sulbactam; CIP, ciprofloxacin; CARBA, carbapenem; TGC, tigecycline; AMINO, aminoglycosides.
![]()
Discussion
A. baumannii has emerged as one of the leading causes of nosocomial infections in critically ill patients in ICUs. Resistance of A. baumannii isolates to carbapenems is an increasing problem worldwide [235]. Our data, in agreement with several recent Greek and international studies, showed the proportion of carbapenem-resistant clinical isolates in our institution to be close to 93%. Notably, with the exception of colistin, none of the antibiotics tested demonstrated in vitro efficacy against A. baumannii.
In a recent study of 441 bloodstream isolates of A. baumannii recovered over an 8-year period from the University Hospital of Patras, the largest tertiary hospital in Southwestern Greece, 92.1% were resistant to ≥3 and 79.4% were resistant to all but one or two classes of antimicrobials [11]. Resistance to ampicillin/sulbactam, meropenem, gentamicin, ciprofloxacin, minocycline, and tigecycline increased significantly over time in that study, while no isolate was colistin resistant [11]. In a recent report from St. Paul General Hospital of Thessaloniki in Northern Greece, the resistance rate of A. baumannii ICU isolates to carbapenems was 84.61% compared to 65.78% in non-ICU isolates. In the same hospital and time period, resistance to gentamicin among carbapenem-resistant isolates was 88% [12].
Acquisition of MDR A. baumannii in ICU patients is strongly related to colonization pressure. A recent study from an ICU in a General University Hospital of Northern Greece showed strong colonization pressure, with more than two carriers per week admitted for hospitalization to independently increase the acquisition risk of MDR A. baumannii [13]. In an older study of 680 adult patients hospitalized in a surgical ICU of a tertiary hospital in Athens, all isolates of A. baumannii were susceptible to colistin; however, multidrug resistance was found in 45% of these isolates [14].
It is notable that the evolution of A. baumannii isolates in Greece, from carbapenem-susceptible in the 1990s to carbapenem-resistant in the 2000s, was rapid. Resistance to imipenem increased from 0% in 1996 to 91% in 2006 among A. baumannii isolates obtained from patients hospitalized in ICUs of Greek hospitals [15]. In the European component of the Regional Resistance Surveillance Program, a total of 21 countries, including Greece, were monitored for antimicrobial resistance patterns of various pathogens. In 2011, Acinetobacter clinical isolates (86% A. baumannii) were generally MDR, with only colistin (99.2% susceptibility of isolates) and tigecycline (95% susceptibility) showing significant antimicrobial activity [16]. All other tested antimicrobial agents exhibited <50% susceptibility, except for cefoperazone/sulbactam (52.5%), which is not commercially available in Greece, doxycycline (51.6%), and tobramycin (59.1%) [16].
From 1999 to 2009 A. baumannii strains carrying the blaOXA-58 carbapenemase gene predominated among carbapenem-resistant isolates in the hospital flora of various Mediterranean countries, including Greece [17]. Since 2009, A. baumannii isolates that carry blaOXA-23 and produce OXA-23 carbapenemase have been increasingly reported; these strains severely limit the treatment options available [518]. The widespread circulation of these strains, which belong to international clonal lineages I and II, seems to reflect a global trend [18].
In our study and for 13 of 14 antibiotics for which a significant difference in the susceptibility rates by hospital unit origin was noted, ICU A. baumannii isolates showed the highest rates of resistance followed by those from surgical or medical wards. Interestingly, this was not the case for colistin, for which surgical wards isolates were more resistant than either ICU or medical wards isolates. However, since the number of colistin-resistant strains was small, especially those derived from medical wards, we cannot reach any definitive conclusions.
Sulbactam, a β-lactamase inhibitor, used to be effective. It was even more effective than carbapenems or polymyxins against A. baumannii infections [1920]. Unfortunately, our in vitro results showed a resistance rate of >92% to this antibiotic.
Our A. baumannii strains demonstrated resistance towards gentamicin and tobramycin that increased through time. On the other hand, 57.7% of the clinical isolates from 2013 and 2014 were susceptible to amikacin, which, anecdotally, has been used successfully in combination with colistin, tigecycline, or sulbactam in cases of difficult-to-treat infections. However, A. baumannii blood isolates from Greece collected in February 2006 and reported to the MYSTIC (Meropenem Yearly Susceptibility Test Information Collection) program showed an 87.3% resistance rate to amikacin [5].
The in vitro activity of ciprofloxacin against A. baumannii strains of our hospital was also less than expected, with an overall resistance rate of 93.3%. Prior exposure to ciprofloxacin has been associated with the development of bacteremia due to resistant gram-negative bacilli, including A. baumannii [21].
We noted rising susceptibility rates of A. baumannii isolates to trimethoprim/sulfamethoxazole over the study period, likely because of the limited use of this bacteriostatic agent in recent years. However, the overall rate of resistance to trimethoprim/sulfamethoxazole throughout the study period was 63.57%. In a very recent survey describing secular trends in resistance of 39,230 A. baumannii respiratory and bloodstream isolates in the United States from 2003 to 2012, the rate of resistance to trimethoprim/sulfamethoxazole was 55.3%, the second highest rate behind resistance to doripenem [22]. Although trimethoprim/sulfamethoxazole has not traditionally been recommended for the treatment of MDR Acinetobacter infections, it might be considered in combination with other agents when limited therapeutic options exist [23].
Regarding tigecycline, a semi-synthetic broad-spectrum glycylcycline, we noted an increase in resistance of A. baumannii strains in later years of the study. Comparable results were reported by Spiliopoulou et al. In their study, tigecycline resistance was low during the first 4 years of their study (2006–2009) (25.5%), but increased up to 66.5% during the last 4 years (2010–2013) [11]. Although not formally evaluated, the rising resistance of A. baumannii to tigecycline in our hospital is likely related to the widespread use of this antibiotic in recent years, in and out of the ICU, for difficult-to-treat gram-negative infections other than A. baumannii and P. aeruginosa, because its use for these pathogens is off-label (A. baumannii) or not indicated (P. aeruginosa). Moreover, several studies have reported poor clinical outcomes with tigecycline therapy in MDR A. baumannii infections [2425].
Colistin is regarded as the most effective antibiotic for MDR A. baumannii [2627]. In fact, it is frequently the only therapeutic option for extensively drug-resistant strains. Therefore, it is worrisome that 7.9% of our A. baumannii clinical isolates were resistant to colistin in 2014. This figure is higher than has been reported from other Greek hospitals in recent years. For example, in the Regional Resistance Surveillance study, colistin-resistant isolates were detected in 3.7% of cases in Greece [16]. A slightly lower rate was reported by Souli et al., with 3% colistin resistance observed in 100 A. baumannii strains collected between September 2003 and November 2005 in 17 tertiary-care hospitals of Athens [28]. In a recent matched case-control study that evaluated risk factors associated with the isolation of colistin-resistant A. baumannii, the only independent risk factor identified was previous use of colistin [29]. Hence, the emergence of colistin resistance in our hospital is likely related to selection pressure from excessive colistin use, as shown previously with Klebsiella pneumoniae [5].
A major limitation of our study was that we did not perform molecular epidemiological studies because of the severe financial constraints our institution and Greece is facing presently. Hence, questions regarding the origin, clonal relationship, and nosocomial spread of these pathogens cannot be answered. However, multilocus sequence typing of A. baumannii strains collected in recent years from patients admitted to a general hospital of our area showed carriage of both blaOXA-23 and blaOXA-66 to be prominent [30]. Another limitation of our study was that we did not investigate risk factors associated with acquisition of MDR A. baumannii. Prolonged ICU stay, need for dialysis, increased Pittsburgh bacteremia score and use of carbapenems have repeatedly been shown in other studies to be independent risk factors for acquisition of MDR A. baumannii among hospitalized patients [3132]. Finally, the definition of MDR that we used, i.e., resistance to ≥ 3 classes of antimicrobials, is arbitrary. In 2012, an international expert panel published interim standard definitions for acquired bacterial resistance, but these recommendations rremain controversial [33].
In conclusion, the overwhelming majority of A. baumannii clinical isolates in our hospital are MDR, as it is the case with most Greek hospital currently. It is clear that the remaining therapeutic options for critically ill patients who suffer from A. baumannii infections are extremely limited, and that A. baumannii has started to develop resistance even against colistin. Meticulous hand hygiene by the hospital’s personnel, widespread and appropriate use of cultures, efforts to distinguish colonization from true infection, and avoidance of antibiotic overconsumption by prompt de-escalation of therapy as soon as culture results are available should be implemented in every hospital unit. Finally, given the lack of available therapeutic options for MDR A. baumannii infections, well-controlled clinical trials of combinations of existing antibiotics are urgently needed.
 XML Download
XML Download