

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Bacteremia is identified in approximately 20% of febrile neutropenic patients [1]. Because empirical antibiotic therapy targeting the common and virulent pathogens is important for febrile neutropenic patients [1], continuous surveillance of the causative bacteria of bacteremia in febrile neutropenic patients should be conducted. In the 1960s and 1970s, most cases of bacteremia in febrile neutropenic patients were caused by Gram-negative bacilli, such as Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa [23]. However, bacteremia caused by Gram-positive cocci increased in the 1980s with the introduction of fluoroquinolone prophylaxis, widespread use of central venous catheters, and use of potent anticancer chemotherapy causing severe mucositis [234]. Such a change was also observed in our hospital: 57.4% of bacteremia cases in febrile neutropenic children were caused by Gram-positive bacteria (GPB) in 2009 [5].
Recently, bacteremia due to Gram-negative bacteria (GNB) increased again [2678]. This increase in GNB infections appears to be associated with increases in fluoroquinolone-resistant GNB that have arisen from a wide application of fluoroquinolone prophylaxis, extended-spectrum β-lactamase (ESBL)-producing Enterobacteriaceae, multidrug-resistant (MDR) P. aeruginosa and Acinetobacter baumannii [2]. Therefore, the frequency of antibiotic-resistant (AR) bacterial infections as well as the distribution of the causative bacteria of bacteremia diagnosed in febrile neutropenic patients should be determined. We previously reported the frequency of ESBL-producing strains and their impact on prognosis in febrile neutropenic children with E. coli and K. pneumoniae bacteremia [9]. Although 34.4% of the identified E. coli and K. pneumoniae strains produced ESBL, a significant impact on prognosis was not observed [9]. However, reports on the frequency and clinical impact of AR bacteria other than ESBL-producing E. coli and K. pneumoniae were scarce in children with febrile neutropenia and bacteremia [10]. The present study aimed to identify the distribution of causative bacteria and the proportion and clinical impact of AR bacteria in bacteremia diagnosed in febrile neutropenic children after 2010.
Materials and Methods
1. Patients and study design
The medical records of children ≤19 years of age, who were admitted to Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea, between January 2010 and December 2014 were retrospectively reviewed. Among them, febrile neutropenic children with underlying hematological/oncological disorders who were diagnosed with bacteremia were enrolled in the present study. Seoul St. Mary’s Hospital is a university-affiliated tertiary teaching hospital that has a separate 46-bed ward for children with hematological/oncological disorders. A mean of 1,400 children are admitted to the ward annually, and a total of 346 allogeneic and autologous hematopoietic cell transplantations were performed during the study period.
In our hospital, empirical antibiotic therapy for febrile neutropenic children has been performed in accordance with the recommendations of the committee for “Guidelines for the Empirical Therapy of Neutropenic Fever Patients based on Literature in Korea” [11]. In the presence of neutropenia, prophylaxis with oral trimethoprim/sulfamethoxazole (150 mg trimethoprim/m2 once daily, three times weekly) against Pneumocystis jirovecii was administered, but fluoroquinolone prophylaxis was not given. When febrile neutropenia occurred, empirical antibiotic therapy with piperacillin/tazobactam and isepamicin was started, and a reassessment was performed 3−5 days later. If the causative pathogen was identified, the antibiotics were adjusted accordingly. If the fever persisted without the identification of a definite cause, meropenem was administered as a second-line empirical antibiotic agent. Glycopeptides were added based on the recommended indications [11], and antifungal therapy was started based on the results of serum galactomannan tests and chest imaging studies. The first-line empirical antibiotic agents were changed from piperacillin/tazobactam and isepamicin to cefepime in children with underlying acute myeloid leukemia (AML) in January 2013; however, piperacillin/tazobactam and isepamicin combination therapy was continued in the remaining children. Although neither antibiotic cycling nor antibiotic mixing has been recommended as a strategy to reduce antibiotic resistance [12], the antibiotic change was performed in preparation of the presumable effect of antibiotic heterogeneity on reducing antibiotic resistance in our hospital.
Demographic data including sex and age, and clinical data including the type and status of the underlying hematological/oncological disorders, duration of neutropenia and fever, and the occurrence of severe complications and death were evaluated for the enrolled children. The annual distribution of causative bacteria and proportion of AR bacteria were compared. The frequency of severe complications and mortality were compared between children infected by AR bacteria and those infected by non-AR bacteria to determine the clinical impact of AR bacterial infection. The present study was conducted in accordance with the Declaration of Helsinki. This study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital, and the need for informed consent was waived (Approval number: KC16RISI0244).
2. Microbiological tests
Blood samples for culture were withdrawn using a sterile technique from a peripheral vein and each lumen of a central venous catheter. Each 1−3 mL of the blood samples was immediately inoculated into a culture bottle (BD BACTEC™ Peds Plus Culture Vial, Becton Dickinson, Sparks, MD, USA) and an automated culture system (BACTEC™ FX, Becton Dickinson, Sparks, MD, USA) was used. Bacterial identification and antibiotic susceptibility tests were performed using an automated system (VITEK®2, bioMériux, Hazelwood, MO, USA).
3. Definition
Fever was identified when the tympanic membrane temperature was >38.0ºC or axillary temperature was >37.5ºC [11]. Neutropenia was identified when the absolute neutrophil count (ANC) was <500/mm3 or the ANC was expected to be <500/mm3 within 2−3 days [11]. Bacteremia was diagnosed when at least one blood sample collected during febrile neutropenia grew any bacteria. Normal skin flora, such as coagulase-negative staphylococci (CNS), Bacillus spp., and Corynebacterium spp., were considered true pathogens in cases of the presence of an intravascular catheter and the initiation of antimicrobial therapy [13]. If bacteremia was diagnosed within 1 month after the completion of antibiotic therapy for bacteremia caused by the same pathogen, it was considered incomplete eradication of the previous infection and not included as a separate episode of bacteremia. A polymicrobial infection was identified when two or more species of pathogens grew from a same blood sample or separate samples collected on the same day.
Severe complications included hypoxia, shock, renal dysfunction, hepatic dysfunction, intensive care unit admission, receiving mechanical ventilator care, and death. Hypoxia was defined as an SpO2 <90% identified using a pulse oximeter, while shock was defined when the patient showed a systolic blood pressure <5th percentile of an age-matched normal range and received volume expansion or inotropic agents to raise blood pressure [14]. Renal dysfunction was diagnosed when a serum creatinine level was increased to more than two times of that checked before febrile neutropenia [15]. Hepatic dysfunction was diagnosed when a serum aspartate transaminase or alanine transaminase level increased to more than two times of that checked before febrile neutropenia with a serum total bilirubin level ≥2.0 mg/dL and a prothrombin time international normalized ratio ≥1.5 [16]. Overall mortality included death of any cause within 30 days after the diagnosis of bacteremia [17]. Mortality due to bacteremia was defined when the patient died within 1 week after the diagnosis of bacteremia without clinical improvement or bacterial eradication from the blood [17].
Methicillin-resistant Staphylococcus aureus (MRSA), methicillin-resistant CNS (MRCNS), and vancomycin-resistant Enterococci (VRE) among GPB and ESBL-producing E. coli and Klebsiella spp., carbapenem-resistant Enterobacteriaceae (CRE), MDR P. aeruginosa, and carbapenem-resistant A. baumannii (CRAB) among GNB were defined as AR in the present study. MDR among P. aeruginosa was defined when the identified strain was non-susceptible to more than three of eight categories of antibiotics recommended to be tested [18].
4. Statistical analysis
The annual distribution of causative bacteria and proportion of AR bacteria were compared using a chi-square test. Clinical factors and the frequency of complications and mortality rates between children infected by AR and non-AR bacteria were compared. Continuous factors were compared between groups using a Mann-Whitney test and categorical factors were compared using a chi-square test. A multivariate analysis using a binary logistic regression test was performed to identify risk factors for AR bacterial infection. Factors showing a P value <0.10 between the two groups on univariate analysis were assessed for association with AR bacterial infection through a multivariate analysis. The statistical analysis was performed using SPSS Statistics 17.0 (SPSS Inc., Chicago, IL, USA), and statistical significance was defined as a two-tailed P value of <0.05.
Results
1. Characteristics of febrile neutropenic children diagnosed with bacteremia
During the study period, 336 episodes of bacteremia were diagnosed in 186 febrile neutropenic children. The median age of the enrolled children was 11 years (range: 0−18 years), and 207 (61.6%) episodes were diagnosed in boys (Table 1). AML (n = 150, 44.6%) and acute lymphoblastic leukemia (ALL; n = 112, 33.3%) were the most frequent underlying hematological/oncological disorders. Consolidation chemotherapy (n = 126, 37.5%) was the most common therapy administered prior to the development of bacteremia. Re-induction or palliative chemotherapy was administered in 155 (46.1%) episodes prior to bacteremia, and 57.6% of the bacteremia episodes in children with malignancies occurred during non-complete remission or response (CR) states.
Table 1
Characteristics of febrile neutropenic children diagnosed with bacteremia

Data are numbers (%).
aThere were no administered therapy prior to the development of febrile neutropenia in 11 episodes (Nine episodes of severe aplastic anemia and two episodes of non-malignant hematological disorder).
bThe remission states of underlying malignancies were determined in 316 episodes except for 20 episodes with underlying severe aplastic anemia or non-malignant disorders.
![]()
Fever persisted for a median of 3 days (range: 1-99 days), and severe complications occurred in 94 (28.0%) episodes (Table 1). Oxygen administration (n = 80, 23.8%) and septic shock (n = 47, 14.0%) were most common among severe complications. A total of 63 children (18.8%) died within 1 month after the diagnosis of bacteremia, and 31 (49.2%) of them died due to bacteremia.
2. Periodic change of the distribution of causative bacteria and antibiotic-resistant bacteria
During the whole study period, GNB and GPB caused 181 (53.9%) and 155 (46.1%) episodes of bacteremia, respectively (Table 2). The annual proportions of GNB and GPB were significantly different (P = 0.049). The proportion of GPB in 2010 was similar to that in 2014 (P = 0.292) and significantly higher than those in 2011−2013 (P = 0.010); however, there were no significant differences from 2011 to 2014 (P = 0.391). Viridans streptococci (n = 87, 25.9%), Klebsiella spp. (n = 56, 16.7%), and E. coli (n = 55, 16.4%) were the most frequent causative bacteria (Table 2). The overall distribution of causative bacteria was not significantly different annually. Enterobacter spp. showed a significant change in the proportion in bacteremia (P = 0.042); however, it accounted for only 3.3% of bacteremia during the whole study period.
Table 2
The annual distribution of causative bacteria in bacteremia of febrile neutropenic children
Data are numbers (%).
GNB, gram-negative bacteria; GPB, gram-positive bacteria; CNS, coagulase-negative staphylococci.
![]()
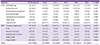
AR bacteria were identified in 85 (25.3%) episodes, and the frequency of AR bacteria was not significantly different annually (Table 3). ESBL-producing E. coli and Klebsiella spp. were most common among AR GNB, and they accounted for 30.6% of the identified E. coli and K. pneumoniae. ESBL-producing strains were 30.9% of E. coli and 30.4% of Klebsiella spp., proportions that were not significantly different (P = 0.950). MRCNS was most common among AR GPB, and it accounted for 88.5% of the identified CNS. During the study period, the proportions of each AR bacterium were not significantly different annually.
Table 3
Frequencies of antibiotic-resistant bacteria identified in children with febrile neutropenia and bacteremia during the study period

Data in brackets are the proportion of antibiotic-resistant bacteria to the total identified strains of each bacterial strain.
aThree isolates of carbapenem-resistant Enterobacteriaceae were also positive for the extended-spectrum β-lactamase.
ESBL, extended-spectrum β-lactamase; MDR, multidrug-resistant; CNS, coagulase-negative staphylococci; NA, not available.
![]()
3. Clinical impact of antibiotic-resistant bacterial infection
Significantly more children with an AR bacterial infection received palliative care and were in a non-CR state compared with those with non-AR bacterial infection (Table 1). On multivariate analysis, only the non-CR state of underlying malignancy was a significant risk factor for AR bacterial infection among the type of underlying disorder, administered therapy, and remission state of underlying malignancy (P = 0.047; odds ratio, 5.847; 95% confidence interval, 1.026−33.307).
The frequency of complications and mortality rate were compared between children infected by AR and non-AR bacteria to determine the clinical impact of AR bacterial infection (Table 1). Severe complications occurred more frequently in children infected by AR bacterial than in those infected by non-AR bacteria (P <0.001). Children infected by AR bacteria were prone to receiving oxygen therapy (P = 0.002) and mechanical ventilator care (P = 0.011) and admitting to the intensive care unit (P = 0.017) compared with those infected by non-AR bacteria. AR bacterial infections caused significantly higher rates of overall mortality (P <0.001) and mortality due to bacteremia (P <0.001) compared with non-AR bacterial infections.
In GPB infections, AR GPB infections caused a significantly higher mortality rate compared with non-AR GPB infections; however, mortality due to bacteremia was not significantly different between the two groups (Table 4). Among the GNB infections, AR GNB infections caused significantly higher rates of overall mortality (P = 0.001) and mortality due to bacteremia (P <0.001) compared with non-AR GNB infections (Table 4).
Table 4
Clinical impact of antibiotic-resistant bacterial infection

aP-values were determined between antibiotic-resistant and non-antibiotic-resistant GPB groups.
bP-values were determined between antibiotic-resistant and non-antibiotic-resistant GNB groups.
GPB, gram-positive bacteria; GNB, gram-negative bacteria; ICU, intensive care unit.
![]()
Discussion
In the present study, the causative bacteria of bacteremia diagnosed in febrile neutropenic children after 2010 were investigated. GNB caused 41.8% of bacteremia cases in febrile neutropenic children in our hospital in 2009 [5], while the proportion of GNB increased to 53.9% in the present study. However, a further increase in GNB infections after 2010 was not identified in the present study. AR bacterial infections had a poorer prognosis than non-AR bacterial infections; however, the proportion of AR bacteria among bacteremia cases in febrile neutropenic children has not significantly increased since 2010.
The proportion of GNB in bacteremia diagnosed in febrile neutropenic patients or those with underlying hematological/oncological disorders varied among geographical locations and time periods [26]. GNB caused a median 42% (range: 14−69%) of bacteremia cases in children with hematological/oncological disorders in the 2000s, and the proportion of GNB infections tended to increase after the 2000s [678]. Among the GNB infections, the proportion of AR bacterial infections also tended to increase recently [27810192021]. In Korean children with hematological/oncological disorders, GNB caused 49−62% of bacteremia cases in the 2000s, a higher proportion than in western children [222324]. In the present study, 53.9% of bacteremia cases were caused by GNB, which was similar to the previous results in Korean children; however, it was higher than previously reported proportion of GNB, 41.8%, in our hospital in 2009. In the present study, GPB caused more bacteremia cases than GNB in 2010 and 2014. Although the proportion of GPB was significantly higher in 2010 than in 2011-2014, the proportion of GPB in 2014 was not significantly different from that in 2011-2013. As a result, the overall proportion of GNB in bacteremia of febrile neutropenic children increased again after 2010.
Previous studies on Korean children with hematological/oncological disorders reported that 15−21% of bacteremia due to E. coli and Klebsiella spp. was caused by ESBL-producing strains and 71% of bacteremia due to A. baumannii was caused by CRAB [222324]. In addition, 42−75% of bacteremia cases due to Enterococci were caused by VRE, 29−50% of bacteremia cases due to S. aureus were caused by MRSA, and 82−87% of bacteremia cases due to CNS were caused by MRCNS [222324]. In the present study, MRCNS comprised 88.5% of this proportion, which was similar to previously reported proportions in Korean children (82−87%) and adults admitted to hematology wards in our hospital (92.9%) [25]. However, the proportions of VRE and MRSA decreased to 35.0% and 14.3%, respectively. For AR GNB, the proportion of ESBL-producing E. coli and Klebsiella spp. increased to 30.6% in the present study; however, it was lower than the proportion of 43.7% in adults admitted to hematology wards in our hospital (P = 0.048) [25]. The proportion of CRAB also increased to 87.5% in the present study. Although MDR P. aeruginosa caused 32.1% of bacteremia cases due to P. aeruginosa in the present study, there were no previous comparable data in Korean febrile neutropenic children. As a result, the proportion of AR bacteria cases tended to increase among GNB rather than among GPB; therefore, the strategies for appropriate antibiotic therapy should target the increasing AR GNB proportions. In particular, ESBL-producing E. coli and Klebsiella spp. were the most common pathogens among AR bacteria. An appropriate strategy for carbapenem use for these pathogens should be established.
It is well known that bacteremia due to AR GNB causes prolonged hospitalization and increased mortality because of the inappropriateness of empirical antibiotics against AR GNB [21026]. AR bacterial infections caused significantly more severe complications and higher mortality rates than non-AR bacterial infections in the present study. In particular, AR GNB infections rather than AR GPB infections caused poorer prognosis attributable to bacteremia than non-AR bacterial infections. Fortunately, the mortality rate of febrile neutropenic children with bacteremia in the present study was not higher than that reported previously despite the increased proportion of AR GNB infections. The overall mortality rate of febrile neutropenic children with bacteremia in our hospital was 20.3% between 2004 and 2006 [24], while that of the children in the present study was 18.8%. This result may show the appropriateness of the current strategy for antibiotic therapy in febrile neutropenic children despite increasing AR GNB infection rates. If we consider that there was no significant difference in the annual proportion of AR bacterial infections after 2010 in the present study, the current antibiotic therapy strategy can be maintained.
The present study had some limitations. First, we could not determine the occurrence rate of bacteremia in the whole population receiving anticancer chemotherapy, and the viral etiology of febrile neutropenia was not determined because laboratory studies for viral infection had not been performed for febrile neutropenic children in our hospital. Second, the administered antibiotic agents and their appropriateness for each child were not determined because they were outside the range of the present study. Finally, the results of the present study, which was conducted in a single hospital, may be inadequate to be adopted by all other hospitals. The distribution of causative bacteria and their antibiotic susceptibilities in bacteremia of febrile neutropenic patients are influenced by the AR status of each community and each country as well as strategies of infection control and antibiotic use in each hospital [2]. Therefore, each hospital should be aware of individual data of the causative bacteria and their antibiotic susceptibilities in bacteremia of febrile neutropenic patients. Nevertheless, the present study could be helpful for other hospitals, which use a similar strategy for antibiotic therapy in febrile neutropenic patients or are located in countries with similar antibiotic resistance rates to those of Korea.
In conclusion, the proportion of GNB in bacteremia cases in febrile neutropenic children increased after 2010 in our hospital, and this increase was in parallel with the increase in AR GNB infections, especially ESBL-producing GNB. AR GNB infections caused poorer prognosis compared with non-AR bacterial infections, and therefore, continuous surveillance for changing epidemiology of AR bacterial infections and their clinical impact in neutropenic patients with bacteremia should be performed. In addition, strategies for reducing the occurrence of AR bacterial infections and their spreading in the hospital should be established.
 XML Download
XML Download