

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Enterobacteriaceae family includes Escherichia coli, Klebsiella pneumoniae, Citrobacter freundii, Morganella morganii, Proteus mirabilis, Enterobacter species, and Serratia species, to name a few. They are responsible for various infectious diseases such as intra-abdominal infection, urinary tract infection, bloodstream infection and respiratory tract infection [1]. Carbapenem is the main treatment for severe infections caused by Enterobacteriaceae, because they have various resistance mechanisms to overcome extended spectrum beta-lactam [2]. Recently, carbapenem-resistant Enterobacteriaceae (CRE) has become one of the leading infectious concerns worldwide, resulting in high mortality in infected patients [3456]. In the United States, the first outbreak of CRE was reported in New York in 2003. Since this report, the presence of CRE has increased in healthcare facilities [7]. In Asia, the first case of K. pneumoniae carbapenemase was reported in China in 2004, and more cases have been increasingly detected in Taiwan, Korea, and Singapore [34]. In Korea, most of the reported multi-drug resistant (MDR) microorganisms were found at tertiary referral hospitals, and CRE was also detected predominantly at tertiary hospitals [8910]. However, the prevalence and risk factors of CRE acquisition have not been well described in small or mid-sized community-based hospital settings. Therefore, we performed an analysis of epidemiologic characteristics and risk factors for CRE in a mid-sized community-based hospital in Korea.
Materials and Methods
1. Study design and subjects
We retrospectively reviewed the medical records of all consecutive episodes of Enterobacteriaceae from hospitalized patients at Bucheon St. Mary's Hospital, a 607-bed, university-affiliated, community-based general hospital from January 2013 to February 2014. During the study period, surveillance cultures were not performed. The microbial data were obtained from the clinical microbiology laboratory for the purpose of analyzing the prevalence of CRE and comparing antimicrobial resistance profiles with carbapenem-susceptible Enterobacteriaceae (CSE).
The risk factors for patients with CRE were evaluated by using a case–double control design. The case group included all adult patients (age ≥16 years) who were found to have any CRE organism (hereinafter referred to as the CRE group). Only first positive culture data from patients who had multiple cultures for Enterobacteriaceae organisms were included. The case group was randomly matched to two control groups by sites of culture, time needed to collect a microbiological specimen from admission day (± 6 days), and length of stay (>2 days) [11]. Control group I (hereinafter referred to as the CSE group I) was matched to the identical species of the CRE group. Control group II (hereinafter referred to as the CSE group II) was matched to the different species among Enterobacteriaceae compared with the CRE group.
The clinical characteristics, risk factors for acquisition of CRE, and clinical outcomes of the case group were evaluated by comparing with those of the control groups. The following variables were reviewed from the medical records: age, sex, hospital length of stay, colonization of microorganisms, comorbidities, Charlson comorbidity index [12], use of healthcare facilities, use of invasive devices, antibiotics treatment, morbidity, and mortality. This study was approved by the Institutional Review Board of Bucheon St. Mary’s Hospital with a waiver of informed consent (No. HC16RISI0038).
2. Microbiology
The microbial organism identification and antimicrobial susceptibility profiles were determined using the Vitek 2 system (bioMérieux, Hazelwood, MO, USA) in accordance with the manufacturer’s instruction. Minimum inhibitory concentrations (MIC) for imipenem, meropenem, and ertapenem were determined by CLSI M100-S22 guidelines [13]. Morganella, Providencia, and Proteus species were tested against ertapenem and meropenem rather than imipenem because of their intrinsic resistance to imipenem [14]. CRE was defined as organisms of Enterobacteriaceae showing decreased susceptibility to carbapenems (MIC for imipenem ≥2 µg/mL, meropenem ≥2 µg/mL, or ertapenem ≥1 µg/mL) and resistance to all third-generation cephalosporins regardless of carbapenemase production [1516]. For organisms showing reducing susceptibility to carbapenem, a modified Hodge test was performed [17]. For CRE organisms, a carbapenemase confirmation test was conducted using a combined disc test (Rosco Diagnostica, Taastrup, Denmark) [17].
3. Statistical analysis
To evaluate statistical significance, categorical variables were analyzed using the χ2 or Fisher’s exact test and continuous variables were analyzed using the Student’s t-test or the Mann–Whitney U-test. Statistical studies were performed with the Statistical Package for the Social Sciences version 13.0 (SPSS, Inc., Chicago, IL, USA). For multivariate analysis, logistic regression analysis was used. Variables with a P-value of <0.20, on univariate analysis, were entered into the model selection procedure using a stepwise backward process. Variables were two-sided, and P-values <0.05 were considered statistically significant.
Results
1. Microbiologic data
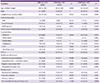
During 229,710 patient-days, 41 (1.6%) isolates of CRE organisms were obtained from among 2,510 Enterobacteriaceae isolates. CRE was cultured from sputum (41.5%), urine (29.3%), surgical wound (17.1%), soft tissue (7.3%), and blood (4.9%). The distribution of CRE species is shown in Figure 1. Only one case of Enterobacter aerogenes showed metallo-β-lactamase based on the combined disc test. Antimicrobial resistance of Enterobacteriaceae is shown in Table 1. In the most cases, the antimicrobial resistance proportions were higher in the CRE group than those of the CSE group. Amikacin and ceftazidime were statistically different between the CRE and CSE groups (P <0.001 and P = 0.024, respectively).

Table 1
Antibiotic resistance of carbapenem-resistant Enterobacteriaceae

CRE, carbapenem-resistant Enterobacteriaceae; CSE, carbapenem-susceptible Enterobacteriaceae; OR, odds ratio; TMP-SMX, trimethoprim-sulfamethoxazole
![]()
2. Demographic data and risk factors for acquisition of CRE
During the study period, a total of 111 patients were enrolled including 37 patients in the CRE group, 37 in the CSE group I (identical species) and 37 in the CSE group II (different species). Four of 37 CSE patients had two species of CRE organisms. CSE group II isolates were comprised of 12 of E. coli, 12 of K. pneumoniae, 5 of Enterobacter cloacae, 3 of Serratia marcescens, 2 of Klebsiella oxytoca, and one each of Citrobacter koseri, E. aerogenes, and M. morganii. The median age of patients in the study cohort was 65.6 years (range, 16–91 years). There were 58 men (52.3%) in the study. The demographic and clinical characteristics of CRE and CSE patients are summarized in Table 2. Based on univariate analysis, the risk factors for acquisition of CRE were MDR Pseudomonas aeruginosa and carbapenem-resistant Acinetobacter baumannii colonization, regular visits to the out-patient clinic, and vascular catheter in CSE group I. The risk factors were MDR P. aeruginosa and carbapenem-resistant A. baumannii colonization, Charlson comorbidity index score ≥ 3, and vascular catheter in CSE group II. The results of multivariate analysis in each control group are shown in Table 3. In CSE group I, regular visits to the outpatient clinic was an independent risk factor for patients with CRE (P = 0.003). MDR species and vascular catheters, however, demonstrated tendencies associated with CRE acquisition (P = 0.056 and P = 0.057, respectively). In the CSE group II, vascular catheter and Charlson comorbidity index score ≥3 were risk factors for CRE (P = 0.010 and P = 0.011, respectively).
Table 2
Patient characteristics according to carbapenem susceptibility of Enterobacteriaceae
aMDR species includes multi-drug resistant Pseudomonas aeruginosa and carbapenem-resistant Acinetobacter baumannii
bRegular visits to the outpatient department are defined as visiting to outpatient department once a month on average
CRE, carbapenem-resistant Enterobacteriaceae; CSE, carbapenem-susceptible Enterobacteriaceae; IQR, inter-quartile range; VRE, vancomycin-resistant Enterococci; MDR, multi-drug resistant; CVA, cerebrovascular accident; CCI, charlson comorbidity index; LTCF, long-term care facility; OPD, out-patient department.
![]()
Table 3
Risk factors for patients with carbapenem-resistant Enterobacteriaceae

aRegular visits to the outpatient department are defined as visiting the outpatient department once a month on average
bMDR species includes multi-drug resistant Pseudomonas aeruginosa and carbapenem-resistant Acinetobacter baumannii
CSE, carbapenem-susceptible Enterobacteriaceae; OR, odds ratio; CI, confidence interval; OPD, out-patient department; MDR, multi-drug resistant; CCI, charlson comorbidity index.
![]()
3. Clinical outcomes associated with CRE
The clinical outcomes of the CRE patients are summarized in Table 4. Those in the CRE group showed more severe disease progression than those of the CSE groups. Only 56.3% patients received susceptible antibiotics for CRE when infection was suspected. The patients with CRE were more likely to experience a reduced level of consciousness, use a vasopressor, be under intensive care, and suffer from acute kidney injury. However, CRE was not an independent predictor of mortality compared with CSE controls. There was no difference in additional hospitalizations in 6 months between case and control groups.
Table 4
Clinical outcomes associated with isolation carbapenem-resistant Enterobacteriaceae

CRE, carbapenem-resistant Enterobacteriaceae; CSE, carbapenem-susceptible Enterobacteriaceae; ICU, intensive care unit.
![]()
Discussion
This case-control study showed the high prevalence of CRE isolates in a mid-sized community-based hospital in Korea. To our knowledge, this is the first study on the prevalence and risk factors of CRE acquisition in the mid-sized community-based hospital in Korea.
The incidence and prevalence of CRE is influenced by geographical characteristics. Mexico and Uganda reported about 10% CRE prevalence [1819]. Asia had a lower rate of CRE (0.6%) [4]. The incidence of CRE in surveillance programs of the general population of the U.S.A. was 2.93 per 100,000 [20]. Previous studies of CRE in Korea showed diverse prevalence. A prospective bacteremia surveillance study of 13 hospitals in Korea showed 3.2% of imipenem-resistant Enterobacter spp., 0.8% of K. pneumoniae and 0.1% of E. coli [21]. From 2005–2008, CRE prevalence was 0.17% at a newly opened intensive care unit (ICU) of a tertiary university-affiliated hospital [22]. In 2012, CRE prevalence of rectal culture surveillance was reported as 0.3% in the ICU of a tertiary university-affiliated referral hospital [13]. However, Kim et al. reported a 7.5% CRE prevalence of stool culture in the ICU of a tertiary university-affiliated referral hospital in 2013 [23]. In our study, the prevalence of CRE in hospitalized patients was higher than expected (1.6%). Our study was conducted at a mid-sized community-based hospital, including not only ICU but also general ward patients. It seems that high transfer rate of long-term care facility patients and greater use of carbapenem in the community-based hospitals may influence the higher prevalence of CRE. Carbapenemase-producing Enterobacteriaceae was only one case by combined disc test in our cohort.
There are a few treatment options for CRE. One of them is tigecycline, which has activity against CRE class A, B, or D enzymes [24]. In Europe, tigecycline showed 88.6% susceptibility against CRE [25]. CRE from the UK had 46.9% susceptibility to tigecycline [26]. In Korea, 3 cases (13.6%) among 22 CRE isolates showed resistance to tigecycline [27]. In our study, 19.5% of CRE isolates were found to be resistant to tigecycline. However, there was no statistical difference between isolates in the CRE and CSE groups.
Several risk factors for the acquisition of CRE have been reported, including previous antibiotics use, vascular device, tracheostomy, admission to ICU, abdominal invasive procedure, chemotherapy/radiation therapy, biliary drainage catheter, and prior hospital stay [32829303132]. Exposure to healthcare facilities is one of the most remarkable risks, especially for long-term care facilities, which are known reservoirs for CRE transmission [33]. Long-term care facility residence was not related to CRE acquisition; however, regular visits to the outpatient clinic was a risk factor for CRE acquisition in CSE group I in our study. Insertion of medical instruments is also a known risk factor for CRE infections [34]. Severely ill patients, such as those undergoing mechanical ventilation, intensive treatment, and transplantation, or those with a lengthy prior hospital stay and course of antibiotics use are at risk for acquiring CRE infection, as reported by a matched case-control study [6]. In our study, vascular catheter and Charlson comorbidity index score ≥3 were the risk factors in CSE group II, as determined by multivariate analysis.
CRE has been reported to affect functional status mortality [5615]. In this study, CRE led to impaired consciousness, transferal to ICU, and risk of acute kidney injury in CSE groups I and II. Patients in the CRE group also showed more frequent use of vasopressor than CSE group II. However, CRE was not related to mortality in either control group. In the present study, only four patients died in the hospital. The small number of patients may not be sufficient for detecting significant differences in evaluating the effect of CRE on mortality. Not all the CRE isolates acted as a pathogen, which may also have influenced mortality.
The present study has some limitations. First, it was a retrospective study. As such, specific information about the type of antibiotics used was missing from the medical records. Second, it included a small number of patients with CRE in a single hospital. Therefore, this result cannot be generalized for the incidence and prevalence of small or mid-sized hospitals in Korea. Third, this study was a case–control design in which the level of risk factors was not equal to the expected level in the population. To minimize bias, we selected two control groups. Fourth, CRE organisms were only examined by a combined disc test for confirmation of carbapenemase. Metallo-β-lactamase and K. pneumoniae carbapenemase were evaluated; however, other carbapenemases could not be investigated. Genotypic confirmation is needed for specification of carbapenemase type.
In conclusion, the incidence of CRE was higher than expected in a mid-sized community-based hospital in Korea. CRE should be considered when a patient has a vascular catheter, high comorbidity score, and regular visits to the outpatient clinic. This study suggests the need for appropriate prevention efforts and constant attention to CRE infection control. A nation-wide investigation pertaining to CRE is needed in community-based healthcare institutes.
 XML Download
XML Download