

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The prevalence of antibiotic resistance in Enterobacteriaceae has increased sharply in recent years [1]. Extended-spectrum ß-lactamase-producing Enterobacteriaceae (ESBL-PE) have become especially common, as ESBL-encoding genes are located on mobile elements that can transfer readily between organisms such as Escherichia coli and Klebsiella spp. [2]. Although traditionally linked to risk factors such as prior hospitalization and antibiotic use, ESBL-PE have become increasingly recognized in the community, especially as pathogens in urinary tract infections (UTIs) [34]. This pattern of community-acquired resistance is concerning, as it may dictate a need for use of broader-spectrum antibiotics when initiating empiric therapy for routine infections [5].
In Sri Lanka, where inpatient and outpatient antibiotic use is widespread and often empiric, the epidemiology of ESBL-PE implicated in UTIs has not been well characterized [678]. No published studies to date have characterized the molecular mechanisms of resistance in ESBL-PE. Therefore, the purpose of this study was to describe the epidemiology of ESBL-PE in UTIs at the largest tertiary care hospital in southern Sri Lanka. Molecular characterization of the ß-lactamase-encoding genes, blaSHV, blaTEM, and blaCTX-M, was performed.
Materials and Methods
1. Selection of bacterial isolates
This was a prospective, laboratory-based surveillance study of patients ≥1 year of age presenting to the largest public, tertiary care hospital in the Southern Province of Sri Lanka. Patients who had a routine urine culture obtained from October 22, 2013 to December 12, 2013 and who, on retrospective chart review, met modified criteria for a UTI as per Centers for Disease Control and Prevention definitions, were included [9]. In patients without urinary catheters or in whom the catheter had been in place for ≤2 days, a UTI was defined as 1) a urine culture positive at ≥104 colony-forming units/mL for ESBL-PE and 2) the presence of at least one sign or symptom such as fever, suprapubic tenderness, costovertebral angle tenderness, urinary frequency, urinary urgency, or dysuria, with onset prior to or on day of urine culture being collected with no obvious alternate cause for symptoms. In patients who had urinary catheters or in whom the catheter had been removed on the previous day, only fever, suprapubic pain, flank pain, and altered mental status were used as potential clinical symptoms indicative of UTI. Community-acquired UTIs were defined using modified Friedman criteria: patients who had urine cultures collected within 48 hours of hospital admission and no history of hospitalization in the prior 3 months, transfer from another hospital, or urinary catheter for >24 hours prior to urine culture collection [10].
2. Antimicrobial drug susceptibility testing and ESBL/carbapenemase detection
Species-level identification and antimicrobial drug susceptibility were determined by Microscan technology according to Clinical and Laboratory Standards Institute (CLSI) guidelines [11]. ESBL production was detected by the double-disk synergy test with cefotaxime (30 µg) and clavulanic acid-amoxicillin (20/10 µg), and confirmed using combined disks containing cefotaxime (30 µg) and clavulanate (20 µg). Minimum inhibitory concentrations (MICs), as determined by microbroth dilution, were also used to verity ESBL production using Microscan technology. A decrease of ≥3 doubling dilutions in the MIC for either cefotaxime or ceftazidime tested in combination with 4 µg/mL clavulanic acid, versus its MIC when tested alone, was considered indicative of ESBL production [12]. The modified Hodge test was performed in isolates with an intermediate or resistant susceptibility profile to ertapenem to detect the presence of carbapenemases [13].
3. ESBL gene detection and typing
DNA extraction was performed for all samples using phenol extraction and ethanol precipitation. The presence of ß-lactamase genes, bla
SHV, bla
TEM, and bla
CTX-M, was detected by polymerase chain reaction as described previously and was confirmed by partial gene sequencing [14].
Ethical approval for this study was obtained from the Ruhuna University Ethical Review Committee and the Duke University Institutional Review Board.
Results
1. Prevalence of ESBL-producing and carbapenem-resistant Enterobacteriaceae
During the study period, 2,192 urine samples were received by the clinical microbiology laboratory. Of these, 1,518 (69.3%) were from inpatients at Teaching Hospital Karapitiya (THK); the remaining samples were from outpatients or patients at a nearby obstetrical/ gynecological public hospital. Of inpatient samples, 18.4% were positive at ≥104 colony-forming units/mL and 184 (65.7% of positives) were Enterobacteriaceae. ESBL production in Enterobacteriaceae was detected in 74 (40.2%) inpatient samples. Retrospective chart review was possible for 47 inpatients, and of these, 38 (80.9%) were thought to have clinically relevant UTIs based on criteria described in the Methods section. The characteristics of these 38 patients and their isolates are described below.
2. Sociodemographic and clinical characteristics
Among 38 patients with UTIs due to ESBL-PE, 5 (13.2%) were <18 years and 16 (42.1%) were male. Thirty-seven (97.4%) patients had symptoms consistent with a UTI on the day of or day prior to admission and 73.7% had urine cultures collected within 48 hours of admission. Traditional risk factors for antibiotic-resistant infections were not commonly reported; in the preceding 3 months, 4 (10.5%) had documented antibiotic use and 3 (7.9%) had documented hospitalization. Nine (23.7%) patients had urinary catheters, with 6 of these placed after onset of UTI symptoms and 3 with unknown dates of placement. Common comorbidities included diabetes mellitus (13, 34.2%), hypertension (7, 18.4%), and a history of recurrent UTIs (4, 10.5%). Overall, 24 (63.2%) UTIs were community acquired based on criteria defined in the Methods section [15].
A total of 35 (92.1%) patients received antibiotic therapy in-house, with UTI or pyelonephritis being documented as a primary medical indication for antibiotics in 88.6% of these patients. Of patients who received antibiotics, 13 (37.1%) were treated with only one antibiotic in-house, 10 (28.6%) were treated with two different antibiotics in-house, and 12 (34.3%) received three or more antibiotics during the course of their hospitalization. The most commonly received antibiotics were third-generation cephalosporins (14, 40.0% of patients who received antibiotics), second-generation cephalosporins (11, 31.4%), aminoglycosides (10, 28.6%), and fluoroquinolones (10, 28.6%). Carbapenems were used in 4 (11.4%) patients. Seven patients (18.4%) were transferred between wards during their stay.
3. Species identification and antimicrobial drug susceptibility
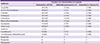
Of 38 patients with UTIs due to ESBL-PE, 36 had cultures that could be further tested for species-level identification and antimicrobial drug susceptibility confirmation. The results for these 36 organisms are listed in Table 1. The majority (30, 83.3%) of isolates were E. coli, with 4 K. pneumoniae and 2 Enterobacter cloacae isolates. All organisms were resistant to ampicillin, cefazolin, and third-generation cephalosporins. Resistance to ciprofloxacin, trimethoprim-sulfamethoxazole, gentamicin, and tobramycin was common among all 3 species. Of tested antimicrobials with clinical utility in UTIs, only amikacin and the carbapenems had greater than 80% susceptibility to these organisms. One E. cloacae isolate had an elevated MIC (2) to ertapenem. The modified Hodge test for this isolate was negative.
Table 1
Species-level identification and antimicrobial drug susceptibilities of urinary Enterobacteriaceae isolates displaying ESBL production among patients with UTIs at a tertiary care hospital in southern Sri Lanka, October to December 2013.
![]()
4. Characterization of extended spectrum ß-lactamase genes
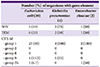
The molecular characterization of the ESBL-PE is listed in Table 2. The SHV gene element was relatively uncommon (3, 10%) in the E. coli isolates and was only found in the presence of other gene elements. The TEM gene element was also uncommon (6, 20%) in E. coli. CTX-M group 1 was present in 27 (90%) of E. coli isolates. Nine E. coli isolates had multiple gene elements in the following combinations: CTX-M groups 1 and 9 (1 isolate); CTX-M groups 1, 9, and 25 (2); CTX-M group 1 and SHV (2); CTX-M group 1 and TEM (3); and CTX-M groups 1 and 9, SHV, and TEM (1). Of the 4 K. pneumoniae isolates, SHV was found in 75% of isolates and TEM was found in 50% of isolates, and CTX-M group 1 was found in all isolates. The 4 K. pneumonia isolates had gene elements in the following combinations: CTX-M group 1 and SHV (1 isolate); CTX-M group 1 and TEM (1); CTX-M group 1, SHV, and TEM (1); and CTX-M groups 1 and 9 and SHV (1). Both E. cloacae isolates had CTX-M group 1, with 1 also having SHV and 1 also having TEM and CTX-M group 25. The E. cloacae isolate with an elevated MIC to ertapenem had SHV and CTX-M group 1 elements.
Table 2
Molecular characterization of ESBL-producing genes in Enterobacteriaceae urinary isolates among patients with UTIs at a tertiary care hospital in southern Sri Lanka, October to December 2013.
![]()
Discussion
Among patients with UTIs at this public, tertiary care hospital in Sri Lanka, the prevalence of ESBL production in Enterobacteriaceae was 40%. The majority of UTIs due to ESBL-PE were acquired in the community by patients who did not have traditional risk factors for antibiotic-resistant infections. Molecular characterization revealed that most isolates possessed ß-lactamases from the CTX-M group 1, which has been associated with the emergence of gram-negative resistance throughout the world [16].
The high prevalence of ESBL-PE is consistent with limited data available from other regions of the country. A prospective, laboratory-based study of uropathogens from a tertiary care hospital in the Western Province revealed that 33% of E. coli and Klebsiella isolates produced ESBLs [7]. A recent report of blood cultures at seven centers nationwide revealed that ESBL-producing E. coli and K. pneumoniae accounted for 23% of cases of clinically relevant gram-negative bacteremia [6]. In hospitals in other South Asian countries, ESBL production among gram-negative urinary isolates can be greater than 60% [1718192021].
The majority of UTIs due to ESBL-PE in our study were acquired in the community. This finding is consistent with those of Dissanayake et al., who reported that 63% of urinary infections due to ESBL-PE in Colombo were community acquired [7]. A growing burden of evidence from throughout the world suggests that community-associated UTIs due to ESBL-PE are increasing in prevalence, with infections being seen in patients who may lack traditional risk factors for antibiotic-resistant infections [522]. In our setting, where oral antibiotics such as amoxicillin-clavulanate, trimethoprim-sulfamethoxazole, and fluoroquinolones can be obtained over-the-counter, many of the isolates were not susceptible to the oral antibiotics tested and the majority of patients were treated with two or more antibiotics during the course of their hospitalization. This may allude to clinicians’ level of uncertainty with treating infections that are potentially antibiotic resistant, especially since confirmation of organism identity and ESBL production generally takes 3 days in this setting, where microbiologic testing is performed manually. Given the need to balance the use of broad-spectrum antibiotics with the need to appropriately treat antibiotic-resistant pathogens, low-cost microbiologic diagnostics that are accurate and rapid are urgently needed.
The majority of ESBL-PE in our study possessed ß-lactamases of the CTX-M-1 group. While a few recent studies have documented the presence of OXA-181, NDM-1, NDM-4, and CTX-M-15 among carbapenem-resistant isolates, to our knowledge, this is the first published molecular characterization of ESBL-PE in Sri Lanka [232425]. The dissemination of CTX-M ß-lactamases, especially CTX-M-15 from group 1, has been associated with the emergence of ESBL resistance worldwide and particularly in community-acquired infections [3262728]. Almost 20% of our ESBL-positive patients were transferred between wards during their hospitalization, which may have implications for infection prevention efforts in this hospital [2930]. Mapping the spread of antibiotic-resistant organisms throughout this hospital, as well as throughout the country and the South Asian region, is needed to better inform infection prevention and control efforts.
Some limitations of this study must be acknowledged. The review of medical records was performed in a retrospective fashion; thus, some charts could not be reviewed and documentation may have been incomplete in others. Further studies with prospective surveillance of antibiotic-resistant organisms and the long-term outcome of patients are needed in this setting.
In conclusion, our study is the first molecular description of urinary ESBL-PE from Sri Lanka, and indicates that ESBL-PE infections that are community acquired are common and associated with the CTX-M group 1 ß-lactamase. Further studies to determine the clinical and molecular epidemiology of antibiotic-resistant gram-negative infections in Sri Lanka are urgently needed to determine the best strategies for prevention and treatment of these infections.
 XML Download
XML Download