

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Antibiotic resistance is a growing threat to public health worldwide [1]. The increase in antibiotic resistance is associated with substantial increases in mortality and morbidity, length of hospitalization, and cost of health care [2]. In 2011 under the theme "Combat Drug Resistance" the World Health Organization (WHO) called for urgent and concerted action by governments and their national partners to halt the spread of antibiotic resistance [3]. A key strategy for limiting antibiotic resistance is antibiotic stewardship [34]. Antibiotic stewardship programs (ASPs) are proven to both optimize antibiotic prescribing and reduce adverse events associated with antibiotic use [5]. ASPs are usually implemented as individual hospital programs targeting antibiotic use for inpatients [6]. Government regulations, so called “administrative antibiotic stewardship”, have also been implemented to improve antibiotic use at the national level in different countries. For instance, Belgium [7], China [8], and France [910] have launched successful nationwide programs promoting improved antibiotic use not only for inpatients but also for outpatients.
In South Korea, antibiotic use in the outpatient setting is high; the proportion of antibiotic prescriptions for acute upper respiratory tract infections (URTIs) is 51·5% to 89·1% in 1990s, which is no less than that in any other countries (about 30% to 80%) [111213141516]. Furthermore, South Korea is known to have a high rate of antibiotic resistance [1].
To promote the proper use of antibiotics and reduce antibiotic costs, the South Korean government has implemented a series of healthcare policies over the last decade. Core elements of these policies were legislative separation of drug prescribing and dispensing, drug utilization reviews, healthcare quality assessment, and public reporting. There have been few reports on the outcomes of these goverment-driven policies so far [1718]. In this review, we describe the administrative antibiotic stewardship policies of the South Korean government and its effects on antibiotic use and resistance.
Evolution of the healthcare system in South Korea
1. Health insurance system
South Korea has a universal National Health Insurance (NHI) system, which has provided greater access for citizens to basic and cutting-edge medical care since the system was introduced in 1989 (Table 1) [192021]. It covers both medical and pharmacy benefits for the entire population. Under the scheme, all office-based physicians dispense drugs in their clinics; the NHI system then reimburses them for the dispensed drugs at pre-determined prices for each drug, thus allowing the physicians to profit on any mark-up over drug purchase costs.
Table 1

![]()
2. Separation of drug prescribing and dispensing
After the introduction of the NHI system, healthcare expenditure continued to rise, and drug spending as a proportion of total healthcare expenditures increased to 26.3% in 2000 [19]. Antibiotics are one of the top drug classes by expenditure. Antibiotic costs accounted for 33.1% of the total pharmaceutical expenditure in 1997 [22]. In the same year, antibiotic use was 33.2 defined daily doses (DDD) per 1,000 inhabitants per day, based on IMS data (IMS Health Korea, Seoul, South Korea), compared with the Organisation for Economic Cooperation and Development (OECD) average of 21.3 [22].
Eventually, in July 2000, the South Korean government implemented a new policy that prohibited physicians from dispensing drugs, and pharmacists from prescribing them. The reform aimed to fundamentally change the inefficient pattern of provision and consumption of pharmaceuticals, to reduce the resultant overuse and misuse of drugs including antibiotics, and to contain pharmaceutical expenditure [2324].
3. Quality assessment of the healthcare service
Concerns arose early on over the possibility of misuse and abuse of antibiotics, injections and high-priced prescriptions, and the health authorities felt it necessary to evaluate the medicines that account for a large proportion of the supply of medications [20]. In July 2000, the National Health Insurance Act was amended to introduce functions for quality assessment of NHI benefit/coverage. The act defines the adequacy assessment service as the duty of the Health Insurance Review and Assessment Service (HIRA), an agency charged with assessing reimbursement of claims under the NHI system. Since then the HIRA has been in control of nationwide quality assessment and has introduced government-driven programs of quality assessment of antibiotic use, as shown in Table 2 [2021].
Table 2
Summary of government-driven quality assessment programs related to antibiotic use in South Korea [2021]

![]()
4. Drug utilization review and public reporting
Initially three categories of outpatient medications prescribed by physicians, comprising antibiotics, injections, and medication costs per day, were evaluated by the HIRA, starting in 2001. The assessment subjects were determined according to the primary diseases (Korean Outpatient Group and Korean Classification of Diseases, Middle Classification) indicated in insurance claims [20]. The indicators for the quality assessment were proportion of antibiotic prescriptions for all diseases and acute URTIs, although national guidelines for the management of URTIs had not been developed. The prescription patterns of all healthcare facilities were analyzed, and feedback about the results was provided to every healthcare facility in an effort to reduce misuse and to promote proper use by strengthening each healthcare facility's autonomy in the use of medications [20]. Antibiotic use for acute otitis media in infants and children since 2012 has been reviewed [21].
Since 2007, the HIRA has publicly reported the results of the quality assessments to help consumers chose hospitals that offer high-quality medical services [25]. The quality indicator results for individual hospitals are posted on the HIRA website.
Effects of the administrative antibiotic stewardship policies
1. Change in antibiotic use for acute upper respiratory tract infections
In the late 1990s, the prescription of antibiotics for diseases that did not need antibiotics was common in outpatient clinics in South Korea. For example, a study of insurance claims in 1994 showed that primary care physicians prescribed antibiotics in 90% or more of adults and children with the common cold and acute bronchitis [11]. The number of antibiotics prescribed was 1.6 per person. In 1999, 51.5% of family physicians prescribed antibiotics for adults and children with the common cold [12].
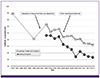
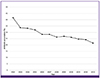
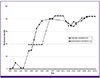
Since the implementation of the new policies, however, the proportion of antibiotics prescribed for acute URTIs has dramatically decreased, as shown in Fig. 1 [111221]. Overall, the proportion of antibiotics prescribed for patients with acute URTI in primary healthcare facilities decreased from 72.9% in 2002 to 42.7% in 2013. As the percentage of antibiotics prescribed for the treatment of acute URTIs decreased, the overall proportion of antibiotics prescribed per total prescription for outpatients also decreased, from 41.6% in 2002 to 21.5% in 2013 (Fig. 2) [2627].
2. Physicians’ perception of antibiotic use for acute upper respiratory tract infections
The perceptions of physicians and pharmacists about antibiotic prescription for acute URTIs have also changed over the past two decades (Fig. 3) [28293031323334]. Studies using clinical scenarios involving the common cold or acute bronchitis showed that physicians’ responses in favor of antibiotic prescription in acute URTIs fell from 75.0% in 1991 to 54.7% in 2003 and to 27.2% in 2010 although the clinical cases and study subjects differed between the studies (Fig. 3A) [282930].
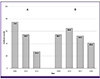 | Figure 3Changes in perceptions of antibiotic use for acute upper respiratory tract infections in South Korea. The perceptions of primary care physicians about antibiotic use for acute upper respiratory tract infection were surveyed using clinical scenarios (A) and standardized patients (B) [28293031323334].
|
Studies using standardized patients with the common cold also confirmed that primary care physicians have prescribed antibiotics less frequently since the separation of drug prescribing and dispensing (Fig. 3B) [31323334]. The decline in antibiotic prescription was more evident after introduction of the public reporting policy.
3. Effect on antibiotic consumption
In short, the separation of drug prescribing and dispensing was the single largest factor to alter overall antibiotic use. The overall proportion of antibiotic prescriptions dropped abruptly after the separation of drug prescribing and dispensing (Fig. 4) [353637]. After implementation of the separation policy, antibiotic use decreased from 28.8 DDD per 1000 inhabitants per day in 1998 to 20.1 in 2002, according to IMS data [35]. The subsequent implementation of public reporting of antibiotic use also led to a modest decrease in antibiotic use for a short period, but it soon started to rise again [37]. According to NHI reimbursement claims data from 2005 to 2009, overall consumption of insurance-covered antibiotics for outpatients decreased from 22.3 DDD per 1,000 inhabitants per day in 2005 to 19.1 in 2007 but then increased to 22.8 in 2009 while change in antibiotic consumption for inpatients was insignificant between 2.3 and 2.5 DDD per 1,000 inhabitants per day during the same period [37]. Most recent data reported to the OECD Health Statistics, including consumption of both insurance-covered and non-insurance-covered antibiotics, have revealed a slowly increasing trend of antibiotic consumption from 26.9 DDD per 1000 inhabitants per day in 2008 to 28.4 in 2012, compared with 20.3 DDD per 1000 inhabitants per day for the OECD mean [38].
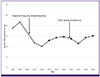 | Figure 4Changes in antibiotic consumption per 1000 inhabitants per day in South Korea before and after implementation of administrative antibiotic stewardship policies including separation of drug prescribing and dispensing and public reporting of antibiotic use, based on IMS data (open circle) [35] and the National Health Insurance reimbursement claims data (filled circle) [3637].
|
Following the reduction of antibiotic use in the treatment of acute URTIs in outpatient services in the last decade, there has also been a fall in the estimated cost of antibiotics used in outpatient services. The estimated reduction in the cost of antibiotics for acute URTIs was 60.8 million US dollars from 2004 to 2007, with a mean of 15.2 million US dollars per year [39].
4. Effect on antibiotic resistance
Little is known about the effect of antibiotic control in the treatment of acute URTIs on antibiotic resistance in South Korea. Rates of beta-lactam and macrolide resistance in Streptococcus pneumoniae have been very high [40]. The rates of penicillin-resistant S. pneumoniae, defined as minimum inhibitory concentrations for penicillin G ≥0.12 mg/L, have been slowly increasing from 0% in 1981 to 77.1% in 2009 (Fig. 5) [4041424344454647]. Resistance to erythromycin also increased from 39.0% to 84.3% over the same period. Meanwhile, the 23-valent pneumococcal polysaccharide vaccine (PPV) was introduced in South Korea in 1991, the pneumococcal conjugate vaccine 7 (PCV7) in 2003, and both PCV10 and PCV13 in 2010 [48]. Because PPV and PCV were only recently included in the national immunization program for older adults (2013) and children (2014), respectively [49], and because of the low rates of PPV vaccination (<6%) [50], it is too early to evaluate the impact of pneumococcal vaccination on pneumococcal resistance.
Discussion
In this review we found a large reduction of antibiotic prescriptions for acute URTIs between 2002 and 2013 in South Korea, and the reduction was consistent across healthcare facilities. These accomplishments resulted from a series of policies launched by the government over the past decade to promote the rational use of antibiotics in healthcare settings. These interventions were unique in that they were mandatory and targeted exclusively healthcare providers including physicians [51].
The proportion of antibiotic use in acute URTIs decreased dramatically after the separation of drug prescribing and dispensing in South Korea (Fig. 1). With the implementation of the policy, the total amount of antibiotic consumption also decreased by one third (Fig. 4). Since the implementation of the public reporting policy, there has been a more sustained decrease in the proportion of antibiotics prescribed for outpatients in all types of healthcare facilities. Despite these decreasing trends, the amount of antibiotic consumption did not fall significantly after the implementation of public reporting (Fig. 4). A sudden drop of the proportion of antibiotic prescription in 2009 (Fig. 1) may be explained by an increase of outpatients with acute URTIs due to the 2009 H1N1 influenza pandemic.
It is of note that measures for improving the quality of care often have unintended consequences [52]. The pendulum could swing towards fewer diagnoses and decreased coding if policies evolve to include public reporting, benchmarking, and financial penalties [5354]. For example, diagnostic transfer was suggested in an earlier study of otitis media in children [55]. Indeed, a study showed a significant change in diagnostic coding after the implementation of public reporting in 2006 [56]. For example, of RTIs for which antibiotics were prescribed, the most common diagnosis was J03 acute tonsillitis in 2005 but changed to J20 acute bronchitis, which has not been designated for antibiotic use evaluation, in 2009 [56]. A rebound in antibiotic consumption since 2008 may be explained in part by this diagnostic shift in the outpatient setting although the cause of increasing trends in total antibiotic consumption needs to be determined. Therefore changes in the frequencies of diagnosis codes for RTIs should be monitored at a regular interval to secure the ongoing effect of these antibiotic stewardship policies.
The government-driven antibiotic policies have mainly focused on the reduction of the antibiotic use in the outpatient setting, as the amount of antibiotic consumption for outpatients is ten times greater than that for inpatients [56]. Surveillance of antibiotic usage is an important component of effective antibiotic stewardship [3]. Data on antibiotic consumption in South Korea are significantly limited. Reported data have been produced using inconsistent methodologies by different groups and organizations, and were not longitudinal but fragmented with a limited time frame. These drawbacks in the surveillance of antibiotic usage make it difficult to assess the change in antibiotic use and to monitor long-term outcomes pertaining to these antibiotic policies.
Certainly these government-driven policies played a pivotal role in improving antibiotic use for outpatients and surgical patients in South Korea. However, some factors need to be considered for these policies to become sustainable antibiotic control programs. First, the interventions were promoted unilaterally by the government under the universal health insurance system in South Korea, and national guidelines for the management of acute URTIs were not developed in parallel with these nationwide interventions. To achieve long-lasting successful outcomes, coordinated efforts and communications among the stakeholders, including physicians and medical societies, are needed. Second, the URTIs designated for drug utilization review also included some bacterial infections, such as acute pharyngitis, tonsillitis, and sinusitis, for which antibiotic therapy is needed when appropriately defined [575859]. Multidisciplinary, coordinated national programs such as the Swedish Strama programme [60] may contribute to a reduction of antibiotic use without measurable negative consequences.
 XML Download
XML Download