

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Gonorrhea is the second most commonly reported communicable disease in the United States, with an estimated incidence of more than 600,000 cases annually [1]. In Korea too, gonorrhea is the second most commonly reported sexually transmitted infection; 3,172 cases were registered by the Korean Centers for Disease Control & Prevention in 2007 [2]. Gonorrhea is usually characterized by cervicitis, urethritis, and pelvic inflammatory disease. Disseminated gonococcal infection (DGI) is an important mucosal infection caused by Neisseria gonorrhoeae but is rare. Classic DGI typically manifests as a combination of dermatitis, tenosynovitis, and migratory polyarthralgia, or as purulent arthritis without skin lesions. Endocarditis, meningitis, and osteomyelitis may also occur but are rare [3]. Here, we report an atypical manifestation of DGI presenting as bacteremia and liver abscesses along with a literature review.
Case Report
A 31-year-old man was admitted to the hospital with periodic fever, skin rashes, and papules on hands, feet, and lower legs as well as pain on the left ankle for the past 20 days. His past medical history was unremarkable. He had been on a business trip to Baengnyeong-do 3 months before admission and had traveled to Tongyeong 1 month before admission. He presented with fever and sore throat 1.5 months before admission and received medication. He did not show any urogenital symptoms such as dysuria or urinary frequency. He was single and heterosexual, and his last sexual contact was 3.5 months before admission. The day before admission, he had visited a dermatologist, at which time a punch biopsy specimen was obtained from a skin lesion on the left sole.
On admission to the hospital, his body temperature was 38.3℃, blood pressure was 130/80 mmHg, pulse rate was 110 beats per minute, and respiratory rate was 20 breaths per minute. Upon physical examination, he seemed to be acutely ill with many hemorrhagic rashes and partly necrotic erythematous papules on both hands and feet (Fig. 1). His white blood cell count was 15,650/mm3 (neutrophil 84.0%), hemoglobin level was 11.5 g/dL, and platelet count was 81,000/ mm3. The erythrocyte sedimentation rate was 94 mm/hour, and C-reactive protein level increased to 8.23 mg/dL. The liver function test results were as follows: aspartate aminotransferase, 24 IU/L (normal range, <40 IU/L); alanine aminotransferase, 34 IU/L (normal range, <40 IU/L); gamma-glutamyl transpeptidase, 82 IU/L (normal range, <50 IU/L); total bilirubin, 0.68 mg/dL (normal range, 0.2-1.1 mg/dL); and direct bilirubin, 0.20 mg/dL (normal range, <0.5 mg/dL). The results of a human immunodeficiency virus antibody test and rapid plasma reagin test were negative. Similarly, hepatitis A, hepatitis B, and hepatitis C serology test results were negative. Chest radiography showed no active lung lesion. Blood, urine, and stool samples were collected for culture. The patient was treated with empirically intravenous ceftriaxone at a dose of 2 g once a day.
On hospital day 2, for evaluation of the fever source, an abdominal computed tomography (CT) scan was performed and fever had subsided. The CT scan results indicated small-sized, low-attenuated lesions with enhancing wall in the liver, and these lesions were considered to be liver abscesses (Fig. 2). On hospital day 3, blood cultures revealed the presence of gram-negative diplococci. On hospital day 7, blood culture organisms were identified as N. gonorrhoeae using a conventional method. Sequencing of 16S rRNA of this isolate indicated the highest homology (99.9%) to the published sequence of N. gonorrhoeae strain NCTC 83785 (GenBank Accession No. NR-026079.1). This isolate was found to be intermediate-resistant to penicillin, resistant to ciprofloxacin and tetracycline, and susceptible to ceftriaxone, cefepime, and cefotaxime using the disk diffusion method.
Histopathology examination of the skin biopsy indicated chronic dermatitis. C3 and C4 complement levels were 125 mg/dL (normal range, 88-201 mg/dL) and 20.6 mg/dL (normal range, 16-47 mg/dL), respectively. Follow-up blood culture was performed before discharge. After 8 days in the hospital, the patient's clinical status was better and he was discharged and prescribed oral cefixime 200 mg twice a day for 2 weeks.
After 2 weeks, the patient visited the outpatient clinic of the infectious disease department. Follow-up blood cultures confirmed the absence of bacterial growth. However, he complained of sweating, pelvic pain, and mild fever (37.5℃); therefore, he was prescribed oral cefixime 200 mg twice a day for 1 week. Three weeks after hospital discharge, his symptoms were resolved and he no longer received antibiotic therapy. The follow-up abdominal CT scan examination after 4 weeks of therapy showed the absence of liver abscesses.
Discussion
DGI results from the bacteremic dissemination of N. gonorrhoeae and affects 1-3% of patients with gonorrhea [4,5,6,7,8,9,10]. In the Korean population, GDI is quite rare, and only 3 cases have been reported to date. In 2004, Kim et al. [11] reported a case of DGI concomitant with acute viral hepatitis C. Kim et al. [12] reported a case of DGI presenting as Sweet syndrome and Won et al. reported the first case of N. gonorrhoeae bacteremia in a 42-year-old man who had hepatitis B virus-associated liver cirrhosis with massive variceal hemorrhage [13] DGI is usually characterized by dermatitis, tenosynovitis, and septic arthritis and rarely by endocarditis, meningitis, and osteomyelitis [11]. The pathogenesis of DGI is associated with both microbial and host factors [14]. The host risk factors for DGI include female gender, pregnancy, menses, asymptomatic mucosal infection, multiple sexual partners, low socio-economic status, intravenous drug use, complement deficiency, HIV infection, and systemic lupus erythematosus [15, 16]. In addition, certain strains of N. gonorrhoeae (ex. Protein 1A serotype, those lacking protein II, and arginine-hypoxanthine-uracil strains) that are prone to cause disseminated infection differ biochemically from more common strains that cause urethral complications; in addition, they are less potent stimulators of inflammatory responses and are less likely to cause symptomatic urethral infections [15]. In this report, microbial factors may have had an important role in the development of DGI because the patient was immunocompetent and had no risk factors for DGI. However, we did not perform further phenotypic or serologic characterization of this isolate.
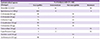
The antimicrobial susceptibility of N. gonorrhoeae isolated from Korea in 2013 is shown in Table 1 [17].
The incubation period of N. gonorrhoeae varies between 1 and 14 days (usually 2-5 days) [18], and hematogenous spread typically occurs within 2-3 weeks of the primary infection [19]. In the case reported herein, the patient's last sexual contact was 3.5 months before admission and symptoms included fever and sore throat approximately 2 months after the last sexual contact. Thus, the incubation period was long but the reason for the long incubation period was unknown. Patients with DGI usually have no urogenital symptoms but do have a history of past venereal infection. It was difficult to identify the causative agent of liver abscesses in this case because they were too small to drain. Therefore, the diagnosis was supported by the evaluation of sexual contact history, clinical symptoms, and bacteremia caused by N. gonorrhoeae.
To the best of our knowledge, this is the first DGI case that presented as liver abscess complications. We performed a literature search to identify previously reported cases of liver abscess caused by N. gonorrhoeae but did not find any case. In general, DGI does not involve abdominal symptoms or signs, and therefore an abdominal CT scan was not necessary in the routine evaluation. Therefore, abdominal complications may occur in the rare cases of liver abscess caused by N. gonorrhoeae. In this regard, in Taiwan, Chung et al. [20] reported the case of a diabetic man with liver abscess due to N. sicca after repeated transcatheter arterial embolization for hepatocellular carcinoma.
In summary, this is the first case of bacteremia with liver abscess caused by N. gonorrhoeae in a young healthy man who had no risk factors for DGI. The patient was successfully treated with 2 g of intravenous ceftriaxone daily for 1 week, followed by 200 mg of oral cefixime twice a day for 3 weeks. Further data will be needed to confirm the involvement of N. gonorrhoeae in the development of liver abscesses.


 XML Download
XML Download