

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Carbapenems have been used as the drug of choice for the treatment of infections caused by multi-drug resistant Gram-negative rods because these drugs easily permeate the porins of outer cellular membranes, exhibit high affinity with penicillin-binding proteins, and are stable against various β-lactamases produced by Gram-negative rods [1234]. However, carbapenem-resistant Enterobacteriaceae (CRE) has appeared as a consequence of the frequent use of these drugs for the treatment of widespread extended-spectrum β-lactamase- and/or AmpC β-lactamase-producing Enterobacteriaceae [5]. Dissemination of CRE is considered a serious clinical threat because available antimicrobials for the treatment of infections caused by CRE are very limited.
Although Enterobacteriaceae can acquire carbapenem resistance via various mechanisms, the most important one is the production of plasmid-mediated carbapenemases [5]. Diverse types of carbapenemases have appeared in Enterobacteriaceae, including 1) KPC- and GES-type enzymes belonging to class A, 2) IMP-, VIM-, and NDM-type metallo-β-lactamases (MBLs) belonging to class B, and 3) OXA-48 and its variants belonging to class D. Enterobacteriaceae strains producing these various carbapenemases have already appeared in Korea [6].
The rapid and accurate detection of carbapenemase-producing Enterobacteriaceae (CPE) in clinical laboratories is essential for the treatment of infections and infection control. However, the identification of CPE strains can be difficult because some CPE clinical isolates exhibit low-level resistance or susceptibility to carbapenems [7]. This study was performed to evaluate the ability of VITEK AST-N202 cards (bioMérieux, Marcy l'Etoile, France) to reliably detect CPE strains isolated from a clinical setting.
Materials and Methods
1. Bacterial strains and susceptibility testing
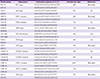
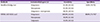
A total of 122 Enterobacteriaceae clinical isolates, 43 CPE and 79 carbapenemase-non-producing Enterobacteriaceae (CNE), were included in this study (Table 1). The CPE clinical isolates were identified as follows: 37 Klebsiella pneumoniae, three Escherichia coli, and three Enterobacter cloacae. The CPE clinical isolates produced KPC-2 (n = 11), KPC-3 (n = 20), GES-5 (n = 5), VIM-2 (n = 2), IMP-1 (n = 1), NDM-1 (n = 2), and OXA-232 (n = 2) carbapenemases. Of the 79 CNE clinical isolates, eight K. pneumoniae isolates were resistant to ertapenem, imipenem, and meropenem, while the remaining 71 isolates were susceptible to these carbapenems; E. coli (n = 35), K. pneumoniae (n = 17), Klebsiella oxytoca (n = 1), E. cloacae (n = 1), Enterobacter aerogenes (n = 6), Enterobacter asburiae (n = 2), Serratia marcescens (n = 4), Citrobacter freundii (n = 1), Citrobacter koseri (n = 1), Morganella morganii (n = 2), and Proteus mirabilis (n = 1). Bacterial species were identified using matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) (Bruker Daltonics, Bremen, Germany) and by analysis of partial 16S rDNA sequences. Antimicrobial susceptibilities of the clinical isolates were determined using VITEK AST-N202 cards (bioMérieux, Table 2). Genes encoding β-lactamases, including TEM-, SHV-, CTX-M-, GES-, and KPC-types of class A; IMP-, VIM-, and NDM-types of class B; CMY-1-, CMY-2-, and DHA-types of class C; and OXA-48-types of class D, were identified by PCR and sequencing (Table 3) [891011].
2. Detection of carbapenemases
Carbapenemases were screened using VITEK AST-N202 cards and modified Hodge tests (MHTs). If an isolate exhibited intermediate or resistance designations to more than one of the carbapenems, ertapenem, imipenem, or meropenem, based on the VITEK AST-N202 card, then the isolate was considered CPE. MHTs were performed with ertapenem and meropenem disks, separately, as described previously [12]. Briefly, a suspension of E. coli ATCC 25922 at a 0.5 McFarland turbidity unit concentration was spread on the entire surface of a MacConkey agar (Becton and Dickinson Company, Sparks, MD, USA) plate. Disks containing ertapenem or meropenem (10 µL, Becton and Dickinson Company) were placed on the center of the agar using a cotton swab, and then the clinical isolates were thickly inoculated from the edge of the disk to the periphery of the agar using a platinum loop. After overnight incubation, if a thickening of the inoculation line of a clinical isolate was observed on the edge of an inhibition zone, then the isolate was considered a CPE strain.
Results
1. Ability of MHTs to identify CPE strains
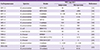
Of the 43 CPE isolates, 35 (81.4%) exhibited positive results in the MHTs with ertapenem or meropenem disks. In the ertapenem MHTs, eight CPE isolates showed false-negative results, including KPC-2-producing K. pneumoniae (n = 1), GES-5-producing K. pneumoniae (n = 2), NDM-1-producing K. pneumoniae (n = 1), GES-5-producing E. coli (n = 1), OXA-232-producing E. coli (n = 1), and VIM-2-producing E. cloacae (n = 2). In the meropenem MHTs, eight CPE isolates showed false-negative results, including KPC-2-producing K. pneumoniae (n = 2), KPC-3-producing K. pneumoniae (n = 1), GES-5-producing K. pneumoniae (n = 1), GES-5-producing E. coli (n = 1), OXA-232-producing E. coli (n = 1), and VIM-2-producing E. cloacae (n = 2). Five CPE isolates showed false-negative results in both ertapenem and meropenem MHTs, including GES-5-producing K. pneumoniae (n = 1), GES-5-producing E. coli (n = 1), OXA-232-producing E. coli (n = 1), and VIM-2-producing E. cloacae (n = 2). All 79 CNE isolates showed negative results regardless of carbapenem susceptibility. Sensitivities of the ertapenem and meropenem MHTs for CPE were both 81.4% (35/43), and that was increased to 88.4% (38/43) when the MHTs were performed with both antibiotics. Specificity of the MHTs was 100% (79/79) (Table 4).
2. Ability of the VITEK AST-N202 card to identify CPE strains
In antimicrobial susceptibility testing using VITEK AST-N202 cards, all 43 CPE isolates exhibited resistance to ertapenem, while only 38 and 41 of the CPE isolates showed resistance to imipenem and meropenem, respectively. Two and three CPE isolates exhibited intermediate and susceptibility patterns to imipenem, respectively, and two isolates were susceptible to meropenem. Three isolates exhibiting susceptibility patterns to imipenem included one GES-5-producing E. coli isolate and two OXA-232-producing E. coli isolates. Two isolates exhibited susceptibility to meropenem, including one GES-5-producing E. coli isolate and one OXA-232-producing E. coli isolate. Of the 79 CNE isolates, eight exhibited resistance to ertapenem, imipenem, and meropenem, while the remaining 71 isolates were susceptible to these carbapenems. Sensitivities to ertapenem, imipenem, and meropenem of the CPE strains when assessed using the VITEK AST-N202 cards were 100% (43/43), 88.4% (38/43), and 95.3% (41/43), respectively. Sensitivity of the VITEK 2 AST-N202 cards for the CPE strains when using all three carbapenems was 100%. Specificities of the three carbapenems for CPE strains using the VITEK AST-N202 cards were all 89.8% (71/79); however, that reached 100% (71/71) when the eight carbapenem-resistant clinical CNE isolates were excluded (Table 4).
Discussion
Although the prevalence of CPE strains is still low (<1%) in Korea, various types of carbapenemases have been identified (Table 4). Since the first isolation of S. marcescens-producing class B VIM-2 MBL in Korea in 2002, VIM-2-producing E. cloacae have repeatedly been reported (Table 5) [13141516171819202122232425]. An outbreak of NDM-1-producing K. pneumoniae sequence type 340 (ST340) was reported in 2012, and the NDM-1-producing E. coli ST101 strain appeared in Korea in 2013 [26]. In a nationwide survey of antimicrobial resistance performed in 2003, a class A GES-5 carbapenemase was first identified in two clinical K. pneumoniae isolates from a hospital in Gyeonggi province, and an outbreak caused by the strain occurred in that same hospital in the next year [19]. Furthermore, a GES-5-producing E. coli ST131 was detected in 2011 [18]. An infection caused by the KPC-2-producing K. pneumoniae ST11 strain was first reported in 2010; thereafter, outbreaks caused by the KPC-2-producing K. pneumonia ST258 strain have been repeatedly reported in several hospitals in Korea [1314]. In 2014, an outbreak caused by K. pneumoniae ST14-producing OXA-232, a variant of class D OXA-48, occurred in a hospital in Seoul, Korea, and E. coli isolates producing this carbapenemase were also detected from rectal swab specimens [25]. Therefore, the development of rapid and accurate methods for the detection of CPE is needed for adequate treatment of infections caused by these microorganisms and for prevention of further dissemination.
Recently, the Clinical and Laboratory Standard Institute (CLSI) recommended MHTs with ertapenem disks as the standard detection method for CPE strains [12]. This study was performed to compare the ability of ertapenem and meropenem MHTs with VITEK AST-N202 cards. Both ertapenem and meropenem MHTs detected 35/43 (81.4%) CPE isolates, and sensitivity was increased to 88.4% (38/43) when the MHTs were performed with both carbapenem disks. The results indicate that the detection of CPE strains is dependent on whether MHTs fail in some cases, especially in cases of CPE strains harboring carbapenemases (GES-5, OXA-232, and MBLs) other than KPC. Ertapenem susceptibility testing using the VITEK AST-N202 card detected all 43 CPE isolates as resistant, while three and two CPE isolates respectively exhibited susceptibility patterns to imipenem and meropenem using this commercial card. CPE isolates harboring GES-5 or OXA-232 exhibited susceptibility to these carbapenems. The results suggest that CPE detection must be conducted based on ertapenem susceptibility when using VITEK AST-N202 cards.
In conclusion, the VITEK AST-N202 card showed excellent performance for the detection of CPE strains. It is recommended that ertapenem-resistant Enterobacteriaceae clinical isolates should be directly subjected to molecular diagnostic methods for the identification of carbapenemase genes, because MHTs did now show sufficient sensitivity for the detection of CPEs.


 XML Download
XML Download