

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Mumps is a common childhood viral disease caused by the mumps virus, and most commonly manifests as swelling of the parotid or other salivary glands. In the pre-vaccine era, mumps was a leading cause of aseptic meningitis and sensory neuronal hearing loss in children. The live attenuated mumps vaccine was first licensed in the US in 1967, and since then, it has been widely used as a component of the trivalent measles-mumps-rubella (MMR) vaccine. The use of two-dose MMR vaccines has long been implemented as a routine pediatric immunization program in many countries. Following the introduction of the mumps vaccine, the mumps incidence has dramatically declined [1]. However, mumps outbreaks still occur among highly vaccinated populations, suggesting waning immunity against mumps in the absence of natural boosting; this has raised concerns about the effectiveness of the current mumps vaccines.
Mumps vaccine was first introduced in Korea in 1980 and was included in the National Immunization Program as the combined MMR vaccine in 1985. A two-dose MMR vaccination at 12-15 months and at 4-6 years of age was recommended in 1997, and became mandatory for school entrance in 2001[2]. As a result, a two-dose MMR vaccine uptake reached up to more than 95% among preschool children in Korea [3]. However, the incidence of mumps has steadily increased since 2007 and sharply rose in 2013 (Fig. 1) [4]. The number of mumps cases continues to rise in an unprecedented scale. In order to identify the causes of mumps epidemic in Korea, new insights into the changing epidemiology of mumps following vaccination are needed.
The changing epidemiology of mumps in Korea
In the prevaccine era, the average age at infection was 4-6 years of age and 90% of children aged 14-15 years were seropositive for mumps virus, indicating that almost all individuals in an unvaccinated population became infected [1]. During this era, mumps epidemics occurred every 4 to 5 years with the peak incidence being in winter and spring in the temperate climate [1]. The introduction of mumps vaccination has changed the epidemiology of the disease and resulted in a significant decline in its incidence, a shift in at-risk populations towards older age groups, and consequent changes in clinical features of mumps. The periodicity of mumps epidemics has not been observed in highly vaccinated populations. Despite the success of mumps vaccination, there have been small and large mumps outbreaks in many countries where populations are routinely vaccinated against mumps [5, 6, 7, 8, 9]. Mumps outbreaks in the US and the UK were notable, where college students aged between 18 and 24 years were predominantly affected [9, 10]. In 2006, mumps outbreaks in the US occurred mainly in college campuses in the Midwest region. Such resurgence was hypothesized to be caused by waning of vaccine-induced immunity and high exposure pressure due to crowded conditions [9]. On the other hand, in the UK, a mumps epidemic in 2005, which involved 56,000 notified cases, resulted from the accumulation of susceptible individuals who missed opportunities of mumps vaccination because those born before 1987 were generally not eligible for routine mumps vaccination and only the combined measles-rubella vaccine was offered to school children aged 5-16 years during the mass catch-up vaccination in 1994 [10, 11].
In Korea, studies on the mumps epidemiology were scarce in the prevaccine era. Although mumps was included in the national surveillance program, underreporting appeared to be substantial in the past. Serological surveys for mumps conducted in the 1970s (1970, 1975, and 1977) showed that more than approximately 80% of the study population were seropositive before the age of 20 years [12, 13, 14], suggesting that most individuals were infected with mumps in pre-vaccine era in Korea. Assuming that 80% of all births had mumps during their lifetime, the number of mumps cases was crudely estimated to be 640,000 per year and the incidence was estimated at 1,985/100,000 population per year in the 1970s in Korea. Routine vaccination against mumps markedly decreased the mumps incidence by 97.5% comparing between the 1970s and 2014 (50.34/100,000 population), although large and small mumps outbreaks occurred sporadically in kindergartens and in primary and secondary schools during the past two decades (Table 1)[15, 16, 17, 18, 19]. From 2007 and 2012, the incidence of mumps cases steadily increased. In 2013, its incidence sharply rose and continues to increase thereafter (Fig. 1)[20]. The 2013-2014 mumps epidemic in Korea is characterized by several distinct features.
Demographically, mumps outbreaks occurred predominantly among middle and high school students aged 13-18 years, with the highest incidence among adolescents aged 15-17 year old. In this population, two-dose vaccine coverage was reported to reach approximately 99% [21]. The age range of affected individuals has become wider than in previous years, and the number of mumps cases appeared to increase in early teens (12-14 year olds) (Fig. 2). However, the proportion of mumps cases in this age group has not changed significantly during the past decade, whereas the proportion of older teens aged 15-19 years increased and that of children aged less than10 years decreased (Fig. 3.). Interestingly, the number of mumps cases also increased in those aged 30 years or older (Fig. 3), which suggests possible transmission of mumps virus to susceptible adults through household contacts [4]. The male predominance is also a distinct characteristic (the male to female ratio is 2.1). In addition, the age-specific gender ratio was more prominent among adolescents (3.78 among 15-19 year-olds) compared with other age groups (1.4 among 5-9 year-olds; 1.3 among 20-24 year-olds) (Fig. 2B) [20]. Geographically, there was a nationwide increase in the mumps incidence. As of 2008, the largest number of mumps cases was reported in Gyeonggi-do, which is densely populated with the population under the age of 20 years being highest. In 2014, a sudden surge in the number of mumps cases was observed in Gwangju and Jeollabuk-do (Fig. 4). Considering the overall population size of each region, the incidence rate over 100,000 population was particularly high in Daejeon (112.51/100,000) and Jeju-do (116.69/100,000) in 2013 and in Gwangju (218.35/100,000) and Jeollabuk-do (244.03/100,000) in 2014 [20]. The mumps incidence showed strong seasonality, with two peaks in spring (from May to June) and late autumn/early winter (from November to December), which coincided with the Korean school terms (Fig. 5). Despite the increased incidence of mumps, disease severity was low and complications were less frequent compared with the cause that occurred two decades ago [22].
Multiple factors are believed to cause the recent mumps epidemic in Korea: waning immunity against mumps over time and the low effectiveness of the mumps vaccine, leading to the accumulation of susceptible individuals above the epidemic threshold; facilitated transmission in school settings; genotype mismatch between the outbreak and vaccine strains; potential misdiagnosis and possible reinfection. Each of these factors is discussed in the following sections.
Suboptimal effectiveness of the mumps vaccines and waning immunity
Outbreaks can occur when the accumulated number of susceptible individuals is greater than the epidemic threshold for a given population. Susceptible individuals tend to accumulate in pockets of low vaccine uptake or when vaccine-induced immunity is imperfect or wanes rapidly. The possible explanations for the accumulation of susceptible individuals in Korea include missed opportunities for a second dose of mumps vaccine, primary vaccine failure following the use of the Rubini strain, and waning immunity in the absence of natural boosting.
Although the uptake for a first dose MMR vaccine was reported to be 80-90%, a second dose vaccine uptake was estimated to be 30% in Korea [23] before the implementation of a mandatory second dose MMR vaccine for school entrance in 2001. Given that mumps vaccine was not included in the catch-up vaccination program in 2001 in Korea, a large proportion of individuals who were born between 1983 and 1993 might not have been offered a second dose of mumps vaccine and remained partially susceptible because one-dose vaccination is less effective in protecting against mumps and immunity wanes rapidly after one-dose vaccine only. The 1983-1993 birth cohort was considered to contribute to the sporadic outbreaks of mumps during the past decade. In addition, the use of the Rubini strain mumps vaccine may be one of reasons for accumulation of susceptible individuals.
1. Effectiveness of the current mumps vaccines
Among the 3 components of MMR vaccine, mumps vaccine is the least effective in eliciting immune responses, and mumps vaccine-induced immunity wanes rapidly [24, 25]. Seroconversion rates after primary vaccination with the Jeryl Lynn strain containing MMR vaccine ranged from 92% to 98% [26]. A second dose of MMR vaccine was reported to be effectively immunogenic. Those who were seronegative prior to the second dose became seroconverted and mumps antibody titers were boosted after receiving a second dose [27]. Despite good immunogenicity of mumps vaccines in clinical trials, their effectiveness was estimated to be low in outbreak settings: 64-66% for one dose and 83-88% for two doses of the Jeryl Lynn strain vaccine [28, 29].
In Korea, five different mumps vaccine strains have been used: Urabe AM9 and Hoshino before 2000; Jeryl Lynn and Rubini strains during 1997-2002; Jeryl Lynn and RIT4385 strains since 2002. The Rubini strain vaccine has the lowest efficacy (0-33%) among the virus strains used for mumps vaccine [28]. After the introduction of the Rubini strain vaccine, numerous outbreaks attributable to primary vaccine failure ensued worldwide [30, 31], which prompted the discontinuation of using the Rubini strain vaccine by WHO in 2002. Consequently, the Rubini strain vaccine was withdrawn from the Korean market in 2002. Considering that the Rubini strain vaccine was used between 1997 and 2002, a certain proportion of individuals who were born between 1991 and 2001 in Korea could have been vaccinated with at least one dose of the Rubini strain vaccine and possibly constituted a majority of susceptible population. Although there is no accurate information about the Rubini strain vaccinees and their immune status, more than one million people are estimated to be vaccinated with at least one dose of the Rubini strain vaccine based on the data retrieved from the Korean immunization registry and the amount of imported the Rubini strain vaccine doses (1,830,000 doses) [32]. Most (85.8%) of these doses were imported during 2001-2002, suggesting that the 2000-2001 birth cohorts and 1995-1998 birth cohorts might have been at increased risk of receiving the Rubini strain vaccine as the first and second dose, respectively.
However, it is notable that a large mumps epidemic occurred in Korea in more than 10 years after discontinuation of the Rubini strain vaccine use and adolescents aged 15-17 years were predominantly affected, whereas mumps outbreaks attributable to the Rubini strain vaccine use occurred among younger children relatively soon after the introduction of the Rubini strain vaccine in other countries [30, 33, 34, 35]. Therefore, waning immunity plays a crucial role in accumulation of susceptible individuals in the recent epidemic, along with primary vaccine failure due to the Rubini strain vaccine use.
2. Waning immunity against mumps
Waning immunity has been hypothesized to contribute to mumps outbreaks in many countries [5, 8, 36, 37]. A study in the US demonstrated that the after a second dose of MMR vaccine, mumps antibody levels declined over a 12-year period to levels similar to those observed before the second MMR vaccination [38]. Similarly, in a Finnish study, mumps antibody titers and the avidity-index for mumps antibodies significantly decreased by 65% and 24%, respectively, over a 20-year follow-up [24]. This same study revealed that the antibody titers (geometric mean titers [GMTs] 685 mIU/mL) of children aged 10-11 years, who were born after the elimination of mumps in Finland and completed a two-dose MMR vaccination 5 years before this study, did not differ from those (GMT 609 mIU/mL) of old children who received a two-dose MMR vaccination 20 years before. These findings suggested that the rapidity of waning immunity could be potentiated by the lack of natural boosting of mumps. With the significant decrease in the mumps incidence following high levels of vaccine coverage, there are limited opportunities for subclinical boosting due to naturally circulating wild-type mumps virus. So far, the longitudinal data about waning immunity against mumps in the Korean population are insufficient. A cross-sectional serological survey conducted in 2006 indicated that seropositivity for mumps virus was low (85.5%) among Korean preschool children aged 4-6 years who received one dose of MMR vaccine at 12-15 months and it steadily decreased over time after a peak (98.5%) following the second vaccination [39]. Although the protective threshold level of antibody is still inconclusive and cell-mediated immune responses seem to play a certain role in protection, neutralizing antibody levels are associated with immunity against mumps and the decline in antibody levels can be a surrogate of the waning immunity. Vaccine effectiveness was also reported to decrease with time after vaccination. Previous outbreak investigations demonstrated that case patients had lower neutralizing antibody titers than non-case patients [40], and the risk of contracting mumps was higher among those who received MMR vaccine more than 10 years before the outbreak as compared with those who received MMR vaccine within 10 years of the oubtreak [37, 41].
Facilitated transmission of mumps in school settings
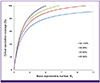
Suboptimal effectiveness and waning immunity may be attributed to the difficulty in obtaining herd immunity for mumps in specific settings with intense exposures. The basic reproductive number (R0) of mumps was estimated to be 4.4 (ranging from 3.0 to 10.3 according to the mixing patterns) based on the data in the prevaccine era [1]. The two-dose vaccine effectiveness was estimated at 85.5% (95% CI 54-96) according to the data from outbreaks in Korean kindergartens in 2006 [16]. On the basis of these estimates, the critical vaccination coverage to maintain herd immunity in Korea is estimated to be 90.5% [42]. However, higher levels of herd immunity and critical vaccination coverage are required to prevent outbreaks as R0 increases and the vaccine effectiveness decreases (Fig. 6). In Korea, adolescents tend to have close interpersonal contacts for a prolonged time in schools. The school hours are long and most students are engaged in after-school activities. The male predominance among mumps cases can be partly explained by the intensity of contacts determined by male students' behaviors and activities. In a setting of high population density and high contact rates, the transmission can be facilitated and the R0 will be higher. Moreover, intense exposure to the virus can overwhelm the vaccine-induced protection against mumps [43]. Although vaccine-induced protection is usually achieved at a particular level of immunity, breakthroughs can occur above this level because of the large challenge dose of the virus [44]. Recent mumps outbreaks among highly vaccinated individuals in Orthodox Jewish communities, where exposure to mumps virus was repeated and prolonged among young boys, or among university students with intense social mixing in crowded living environments are examples of this phenomenon [43, 45]. The finding that seasonality of mumps coincides with the school terms in Korea also indicates the facilitated transmission in school settings. In these settings, two doses of current mumps vaccines may not be effective enough to prevent mumps outbreaks, particularly, when immunity wanes with time after vaccination.
It is concerning that mumps seropositivity among Korean children aged less than 17 years was far below the herd immunity threshold according to a serological survey in 2010 [46].
Genotype mismatch between the vaccine and outbreak strains
Genotype mismatch between the vaccine strain and wild-type mumps virus strains can reduce the protection against outbreak mumps strains [47]. Mumps viruses are categorized into 12 different genotypes (A through N, excluding E and M) based on the sequence diversity in the SH gene, and the dominant genotypes differ geographically [48, 49]. Wild-type viruses currently circulating in the Western hemisphere are predominantly genotype G strains [50], whereas genotype H and I are the most common in Korea [51]. However, the current vaccine strains belong to genotype A (Jeryl Lynn strain) and genotype B (Urabe AM9 strain). Despite this genotype mismatch, immune escape has not been conclusively demonstrated until now. Antibodies induced by the Jeryl-Lynn strain vaccine were shown to neutralize the epidemic strains of different genotypes (type B, C, G and H) [50, 52, 53]. In addition, genotype I mumps virus strains from Korea were neutralized by sera from Jeryl-Lynn vaccinees [54]. However, the neutralization efficiency was lower against outbreak virus strains than against the Jeryl-Lynn strain, suggesting that genotype differences may influence the vaccine efficacy and play a certain role in current mumps outbreaks [47, 55].
Challenges in the diagnosis of mumps
The diagnosis of mumps among vaccinated individuals is challenging. The clinical diagnosis based on classic symptoms of parotitis can be less reliable because these clinical symptoms can be less prominent among vaccinees. Moreover, other infectious agents such as Epstein-Barr virus, parainfluenza virus, adenovirus, and Coxsackie virus can cause similar symptoms [56, 57]. Therefore, laboratory confirmation is important to diagnose mumps cases properly. However, laboratory confirmation is also challenging because of the low sensitivity of currently available diagnostic tests, particularly in highly vaccinated populations. Such a challenge is demonstrated by the fact that only approximately 15% of the cases of 2013-2014 mumps epidemic in Korea were laboratory-confirmed [20]. The most common methods of laboratory diagnosis are virus detection by real-time reverse transcription polymerase chain reaction (RT-PCR) and serological confirmation. However, virus detection by RT-PCR has a low yield with the detection rate being as low as 30% among two-dose vaccinees [58]. The success rate of virus detection can also be affected by the timing of sample collection and sample handling. Clinical specimens should be optimally sampled within the first 3 days of the onset of symptoms and transported in cold storage [59]. The detection of IgM is also low in anamnestic immune responses: IgM was detected in 4-13% of two-dose vaccine recipients [58, 60]. A 4-fold rise in IgG titers in a 2-3 week interval can confirm the diagnosis of mumps; however, paired sera are required and already high IgG titers can reduce the chance of 4-fold rise. For these reasons, a high IgG titer in the serum was suggested as a complementary diagnostic marker for mumps infection among vaccinated patients. Nonetheless, the cut-off of GMT for positivity varied from 5,000 to 25,000 [61, 62]. Moreover, the enzyme immunoassay (EIA) tests are not standardized and have a lower sensitivity than the neutralization test [63]. In addition, most commercial EIA tests for mumps in Korea are non-quantitative and it is necessary to perform end-point titrations to determine if there is a 4-fold or greater difference in titers between acute and convalescent-phase serum samples. In an attempt to improve the diagnostic efficiency, novel approaches have been explored to confirm mumps infection, including capture IgM enzyme immunoassay [64] and ELISpot assay for detecting virus-specific antibody-secreting B cells [65]. Nonetheless, further studies are necessary to standardize these assays for use for mumps diagnosis. As already discussed, false negative results are common in vaccinated individuals. Therefore, laboratory test results should be carefully interpreted and mumps infections cannot be excluded with negative laboratory test results.
Challenges in the control and prevention of mumps epidemics in Korea
Controlling mumps outbreaks is challenging. In order to control the spread of an infectious disease, it is necessary to identify cases, trace contacts, and implement appropriate infection control measures in a timely manner. In cases of mumps outbreaks in school settings, such measures can be less effective because mumps virus can be transmitted during the pre-symptomatic phase or from asymptomatic individuals [59]. In highly vaccinated populations, in particular, the proportion of asymptomatic infections may be larger than the previous estimate of 30% and the early identification of mumps cases can be limited due to the low yield of usual diagnostic tests. For these reasons, the timely containment of mumps outbreaks appears to be more challenging.
Because of the perceived benignity of mumps, mumps outbreaks have gained less attention from the public and infection control measures might have been less stringent even during outbreaks [17]. In a survey conducted during the 2007-2008 mumps outbreaks in Korean high schools, the percentage of mumps cases who were placed in isolation was 40.1% (131/367) and approximately 50% of the respondents (54.5%) reported that they had been instructed on how to prevent mumps transmission when they developed symptoms during outbreaks [17]. Therefore, awareness about mumps should be raised and appropriate hygienic practices should be encouraged in the targeted population at risk, particularly school students.
The occurrence of mumps outbreaks in a highly vaccinated population does not necessarily indicate a failure of routine vaccination programs. Routine mumps vaccination has substantially decreased the incidence of mumps and its complications as compared with the pre-vaccine era [22, 66]. The impact of low vaccine coverage is likely substantial as the estimated annual incidence of mumps ranged from 431,000 to 1,356,000 in Japan, where vaccination against mumps is voluntary and vaccine uptake is less than 30% [67]. In addition, the prompt identification and immunization of high-risk groups is a well-recognized strategy to control vaccine-preventable childhood infections [59]. Therefore, it is important for everyone at risk of mumps infection to up-to-date with two-doses of MMR vaccine. In an effort to control mumps outbreaks, a third dose of MMR vaccine has been provided to high-risk individuals among populations highly vaccinated with two-doses of MMR vaccine [68]. The data currently available are insufficient to recommend for or against the use of a third dose of MMR vaccine for mumps outbreak control. The intervention with a third dose was implemented after an outbreak peak [68, 69]; thus, it is possible that the outbreaks died out on its own. Nonetheless, a third dose mumps vaccine can be used as an outbreak control measure in order to temporarily boost immunity against mumps. Considering that the provision of additional vaccine dose for boosting immunity is one of methods to delay the waning rate of vaccine-induced immunity, the routine use of a third dose against mumps may be necessary to maintain herd immunity in the absence of natural boosting of immunity. However, it is questionable whether a boosting with the currently marketed mumps vaccines can confer long-term protection [47, 70]. More evidence is required to support the routine use of a third dose among high-risk populations, and an economic analysis needs to be performed. More importantly, a more immunogenic mumps vaccine needs to be developed to effectively prevent mumps outbreaks and eliminate mumps in the future.
Conclusion
The mumps epidemic is still an ongoing problem in Korea. The recent resurgence of mumps is a result of multiple factors, and for this reason, multidisciplinary measures need to be taken. The effectiveness of the current mumps vaccines appears to be suboptimal in outbreak settings, and genotypic differences between the vaccine and circulating virus strains have raised concerns about the efficiency of vaccine-induced immunity against the wild-type virus. Nonetheless, the impact of two-dose mumps vaccines should not be overlooked given that routine mumps vaccination has substantially decreased the incidence and its complications. Therefore, the maintenance of high vaccine coverage is an essential element to prevent mumps outbreaks. In addition, better understanding of the mumps dynamics among vaccinated populations and the continuous monitoring of epidemiologic changes are necessary to predict the future epidemics and help develop effective vaccine policies. The disease burden should be evaluated and interventions be economically analyzed on the basis of the empirical data. More importantly, concerted efforts should be made to improve the efficiency of diagnostic tests for mumps and to develop more immunogenic mumps vaccines to better cope with the changing epidemiology of mumps.





 XML Download
XML Download