

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Corynebacterium minutissimum is a gram-positive, non-spore-forming, aerobic or facultative anaerobic bacillus, which is a resident microbe of skin and mucosal membranes. It is the etiologic organism of erythrasma, a common superficial infection of skin [1]. Although some cases of C. minutissimum infection have been reported, it has rarely been a causative agent of invasive extracutaneous infection. To the best of our knowledge, we report on the first case of postoperative abdominal infection caused by C. minutissimum.
Case Report
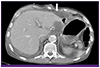
A 76-year-old male patient was referred to the Infectious Division due to high fever and diarrhea. Emergency radical subtotal gastrectomy had been performed 11 days earlier due to occurrence of gastric perforation after endoscopic submucosal dissection of early gastric cancer. After radical subtotal gastrectomy, piperacillin/tazobactam (4.5 g every 8 h) had been administered for treatment of peritonitis. The patient had a medical history of chronic obstructive pulmonary disease without medication. He complained of abdominal discomfort and dyspepsia. On physical examination, he was alert and cooperative. His body temperature was 38.1℃, blood pressure, 130/80 mmHg, pulse, 120 beats per minute, and respiratory rate, 25 breaths per minute. Generalized abdominal tenderness was observed, without rebound tenderness. Blood tests showed a leukocyte count of 42,770/mm3 with segmented neutrophils of 90.2% and a high sensitivity C-reactive protein level of 21.22 mg/dL. His blood, urine culture result showed no growth of bacteria. Findings on abdominal computed tomography showed complicated fluid collection with a small amount of air bubble around the operation site (Fig. 1). Percutaneous catheter drainage was inserted into the peritoneal cavity. Doripenem (500 mg every 8 h) was started empirically.
Gram stain of abdominal drainage showed slightly curved, gram-positive rods. A positive catalase reaction was observed. The specimen was cultured on 5% sheep blood agar plates at 35℃ overnight and identified using the Vitek II Anaerobic and Corynebacterium identification card (BioMérieux, Durham, NC, USA). Final results of culture testing confirmed C. minutissimum. The isolate was susceptible to ampicillin, tetracycline, erythromycin, and vancomycin, but intermediately susceptible to penicillin. Initial empiric doripenem was discontinued and amoxicillin/sulbactam (1 g/500 mg every 8 h) was started and maintained for 23 days, until discharge. Subsequent abdominal CT on the 40th post-operative day showed no complicated fluid. The patient was discharged on the 44th post-operative day.
Discussion
Corynebacterium species are found as colonizers of the skin and other tissues and in the environment. Although pathogenic non-diphtheriae Corynebacterium (Corynebacterium jeikeium, Corynebacterium amycolatum, Corynebacterium urealyticum, and C. minutissimum) have been reported with some frequency, these bacteria are among the micro-organisms that are often neglected by physicians and clinical microbiologists [2]. Among non-diphtheriae Corynebacterium, C. minutissimum remains an uncommon cause of invasive disease. To date, 20 cases of invasive C. minutissimum infection have been reported [3, 4]. These include two cases of peritonitis, both involving patients with peritoneal dialysis [5, 6], and one case of post-surgical abscess in a patient who had undergone cervical discectomy [7]. To the best of our knowledge, we report on the third case of abdominal infection, the second postoperative infection, and the first postoperative abdominal infection caused by C. minutissimum.
Although multi-resistance has been well documented in C. jeikeium [8, 9], C. urealyticum [9], and Corynebacterium striatum [10, 11] strains and in C. amycolatum [12], C. minutissimum is generally susceptible to antimicrobials, including ampicillin, tetracycline, erythromycin, and vancomycin [9, 13]. In our case, the isolate was susceptible to ampicillin, tetracycline, erythromycin, and vancomycin.
Invasive C. minutissimum infection usually occurs in immunocompromised patients and/or patients with skin disruption due to surgery or indwelling devices, such as a central venous catheter and peritoneal dialysis catheter [5, 6, 14, 15]. Although the source of infection was unknown, skin disruption by surgery and drainage catheter might have contributed to development of invasive C. minutissimum infection in this patient.
In conclusion, given an increasing number of cases with non-diphtheriae Corynebacterium as a cause of serious opportunistic infection in immunocompromised patients and the more common use of indwelling devices causing a breach in the skin-barrier [3, 4], clinicians would be wise to keep this organism in mind as a rare cause of post-surgical abdominal infection.
 XML Download
XML Download