

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nontuberculous mycobacteria (NTM) can be categorized into rapidly growing mycobacteria (RGM) and slowly growing mycobacteria (SGM), according to Runyon's classification [1]. RGM are known to have weaker pathogenicity than SGM [2], and they may cause disseminated diseases in skin and soft tissue, pneumonia, and infective endocarditis in immunocompromised individuals [3-6]. Recently, such cases have attracted increasing attention, with infectious diseases caused by NTM being reported in the healthy population [1]. In Korea, there is a slowly growing awareness about the importance of NTM related diseases due to the increased ratio of NTM that are isolated from clinical specimens [7, 8].
The literature in Korea dealing with skin and soft tissue infections caused by RGM consists mainly of single case reports and research results of a single institution. As a result, accurately determining the incidence of such infections is difficult, as there are insufficient numbers of specimens or patient samples to draw on [9]. Most domestic cases of skin and soft tissue infections are caused by Mycobacterium abscessus, Mycobacterium chelonae, and Mycobacterium fortuitum [10], and they are treated according to the guidelines of the American Thoracic Society (ATS) [1]. In order to provide effective treatment for such patients, however, it is necessary to collect data on and analyze domestic cases of RGM infections.
Recently, we experienced 5 cases of skin and soft tissue infections caused by RGM on Jeju Island. Together with these cases, we analyzed all of the skin and soft tissue infections caused by RGM reported to have occurred in Korea thus far. The results are reported in an effort to contribute to domestic epidemiologic data and future clinical treatments.
Methods and Materials
To analyze the characteristics of RGM related skin and soft tissue infections in Korea, we collected data on such infections reported from 1995 to 2011 using the KoreaMed and PubMed databases, as well as included the RGM infected patients in our cases.
The cases were examined at one university hospital in the Jeju Island from January 2003 to May 2012. Over this approximately 10-year span, we saw 6 patients with skin and soft tissue infections caused by NTM, and among these, 5 patients had infectious diseases caused by RGM.
To test for RGM in our cases, we conducted acid fast bacillus (AFB) staining of the samples, cultures of mycobacteria, and polymerase chain reaction (PCR) tests. In cases where NTM were suspected but not identified in the samples and cases where early test results were needed, the mycobacteria species was checked with 16S ribosomal DNA (rDNA) and rpoB gene PCR.
From the domestically reported data, we chose to analyze 24 patients from cases that provided sufficiently detailed information about the isolation of the strains from the specimen, the kind of used antibiotics, the duration of therapy, and the outcome. In the PubMed search engine, there were 2 cases of RGM caused outbreaks [11, 12], and 1 retrospective study [13], but they lacked the data needed for this analysis. In addition, if the 26 patients and the outbreak patients were added, the outbreak data could have been misinterpreted as being infections caused by RGM. Hence, these data were excluded, and the analysis was performed with a total of 15 cases and research papers, along with our cases [9, 14-27].
Results
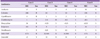
A total of 26 patients were analyzed, including 21 reported cases of RGM caused skin and soft tissue infections from 1995 to May 2012 in Korea and the 5 patients of ours. The analysis results are displayed in Table 1.
The mean age of patients with RGM skin and soft tissue infections was 54 years, and there were 19 females (73%). Thirty percent of the patients had been in contact with water. The route of infection was through procedures performed by medical personnel for 13 patients; acupuncture and bee venom acupuncture for 3 patients; liposuction for 4 patients; fat grafting for 2 patients; percutaneous endoscopic gastrostomy for 1 patient; intra-articular injection and steroid injection for 2 patients; other reasons for 1 patient; trauma for 1 patient; surgery for 2 patients; and foot bath for 1 patient. In the trauma, surgery, and foot bath cases, the infections were caused by a single strain of M. fortuitum complex, while the medical procedure related cases were caused by various RGMs, such as M. abscessus, M. fortuitum complex, M. chelonae, and M. conceptionense. The lesions were located mostly in the upper extremities and lower extremities. Through diagnostic testing, the PCR test showed a positive rate of 77%, and the NTM culture showed 72%. In the isolation of mycobacterium, the M. fortuitum complex was the most common, at 46%. Antimicrobial susceptibility testing was performed on 11 out of the 19 patients. Based on these case reports, rate of mycobacterial resistance to clarithromycin in RGM was 12.5% (1/8), while the mycobacterial resistance rate to quinolone was 60% (3/5). Before 2004, 4 patients among the 8 NTM infected patients were treated with antituberculous agents [20, 22, 27]. Two patients died, including one person who died as a result of using the antituberculous agents [20]. The other patient died because of a systemic illness and comorbidities despite the appropriate use of antibiotics (patient 5). The mean duration for using intravenous antibiotics was 6.7 weeks, and mean total duration of antibiotics use was 21.2 weeks. Regarding the choice of antibiotics, clarithromycin together with a susceptible drug was the most common, accounting for 46% (12/25), while 23% (6/25) were treated with combination of antituberculous agents.
The cases diagnosed at our hospital are as follows (Table 2).
Patient 1: A 71 year old male patient suffered a wound in the left thenar from a screwdriver 4 months before visiting our hospital. For two months before visiting our hospital, the patient had been receiving antibiotic treatment at a local clinic for pain, erythema, and swelling of the injured area. However, as the symptoms did not improve, he visited our hospital (Fig. 1). On the first day, incision and drainage were done, and intravenous first generation cephalosporin was administered. In the magnetic resonance imaging (MRI), multifocal abscesses were observed in the soft tissue of the palm, and the intensity of the signal was increased. In the tissue specimens obtained from the lesion, the gram positive rod was visible. However the AFB stain and the NTM PCR were negative, and the strains did not grow in the NTM culture. Afterwards, M. fortuitum was identified by the 16S rDNA gene and rpoB gene analysis. Hence, a combined antimicrobial treatment regimen of clarithromycin (500 mg every 12 h), ciprofloxacin (500 mg every 12 h), and amikacin (875 mg every 8 h) was used, and the patient improved after 4 weeks of intravenous antibiotic treatment. After discharge, the patient took clarithromycin (500 mg every 12 h) and ciprofloxacin (500 mg every 12 h) for 20 weeks before discontinuing the medication. There were no signs of relapse 4 months after the end of treatment.
Patient 2: A 68 year old female patient had been treated with antibiotics at a local clinic for pain and erythema in the right lower extremities 3 months before visiting our hospital. She came to our hospital because the symptoms did not improve. Tissue biopsy, cultures, and gram staining were performed on the lesion, and an angiography was performed in order to rule out skin ailments caused by vasculitis. There was no evidence of skin infection. Therefore, in suspicion of vasculitis, the patient was treated with a low-dose steroid. While being observed during the treatment, the patient developed an ulcer with discharge from the lesion after having frequently visited a public bath. The gram stains and cultures were repeated on the wound discharge. No organism was isolated, yet weakly positive (+/-) acid-fast bacilli were detected. In addition, pathologic findings revealed chronic inflammatory infiltration in the perivascular, along with granulomatous inflammation in the dermis (Fig. 2). M. fortuitum complex, M. ulcerans, and M. marinum were identified in the NTM culture, and the results of antimicrobial susceptibility testing were as shown in Table 3. The patient received intravenous amikacin (250 mg every 8 h), cefoxitin (3 g every 6 h), oral rifampicin (600 mg every 24 h), and clarithromycin (500 mg every 12 h). After 3 weeks of antibiotics, hepatotoxicity occurred as a adverse reaction to rifampicin; therefore, treatment was changed to oral clarithromycin (500 mg every 12 h) and rifabutin (300 mg every 24 h). One month after hospital discharge, improvement in the lesion was observed, and the medication was changed to clarithromycin (500 mg every 12 h) and moxifloxacin (400 mg every 24 h) for 14 weeks of treatment. For 2 months after treatment, the patient was under observation with no relapse.
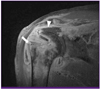
Patient 3: A 72 year old male patient visited our hospital complaining of pain and discharge in the right shoulder, which had started 5 days before. One month before visiting the hospital, the right rotator cuff had ruptured, and the patient had undergone a right rotator cuff reconstructive operation with arthroscopy he had been discharged from hospital without any complications. Two weeks before coming to our hospital, the patient had been to a public bath, and an incision and drain had been performed at a clinic 2 days before hospitalization. The patient was hospitalized for injection therapy. There was erythema, swelling, and discharge on the right shoulder, along with pain and warmth. In the MRI of the right shoulder taken on the first day at the hospital, the intra-articular synovial membrane was thickened, and the signal intensity had increased. The amount of synovial fluid increased, and the supraspinatus muscle and infraspinatus muscle were ruptured (Fig. 3). From the tissue specimens obtained from the lesion, the gram-positive rod was visible, the AFB stain was positive (1+). The NTM PCR was positive and M. fortuitum complex was isolated in the NTM culture. Based on these results, antibiotic treatment was started with clarithromycin (500 mg every 12 h), amikacin (200 mg every 8 h), and cefoxitin (3 g every 6 h). The results of antimicrobial susceptibility testing after 4 weeks were as shown in Table 3. Because inducible resistance to clarithromycin was revealed in this test, clarithromycin was changed to doxycycline. As improvement occurred in the lesion area afterwards, the treatment was finished after maintaining oral doxycycline (100 mg every 12 h) and moxifloxacin (400 mg every 24 h) for 24 weeks. The patient has been under observation at the clinic for 3 months with no relapse.
Patient 4: A 71 year old female patient suffering from right shoulder pain had gone to a local clinic for relief 10 days before visiting the hospital. Six weeks before visiting the hospital, the rotator cuff of her right shoulder had ruptured, and she had undergone rotator cuff muscle repair. The patient had been discharged from hospital after surgery without any complications. Ten days before visiting the hospital, the patient had experienced pain, wound dehiscence, and discharge at the operation site, and she had been treated at a local clinic. The patient had been in contact with water at a public bath 2 weeks before visiting the hospital, and the lesion had worsened at that time. The day after the patient came to the hospital, incision and debridement were performed on the right shoulder, and a culture study was performed on the pus and tissue. From the tissue specimen taken from the operating room, we found gram positive, the AFB 1+ bacilli. In the tissue culture study 1 week later, M. fortuitum complex was isolated. Clarithromycin (500 mg every 12 h), amikacin (200 mg every 8 h), and cefoxitin (3 g every 6 h) were administered. The results of antimicrobial susceptibility testing were as shown in Table 3; antibiotics were intravenously injected for 4 weeks. Because there was improvement in the lesion area, oral clarithromycin (500 mg every 12 h) and moxifloxacin (400 mg every 12 h) were maintained for 20 weeks before discontinuing the treatment. The patient has been under observation at the clinic for 4 months with no relapse.
Patient 5: A 78 year old female patient who had been suffering from a pain-accompanied wound in the left foot went to a clinic for examination 10 days before visiting our hospital. At the time of visiting our hospital, there were multifocal ulcers. Fascia and muscle were exposed in the left foot. There was no history of trauma, and the patient frequently used the public bath. In the medical history, the patient was taking aspirin, valsartan, atorvastatin, isosorbide dinitrate, furosemide, and levothyroxine for primary hypothyroidism and congestive heart failure caused by hypertension and valve insufficiency. The patient was also taking prednisolone 7.5 mg for adrenal insufficiency. At the time of the patient's visit, the wound was presumed to be a general skin infection; therefore, we started empirical antibiotic therapy with ampicillin/sulbactam. The specimen taken from the lesion area revealed gram-positive rod. Pseudomonas was confirmed in the culture study, and AFB stain was positive (4+). Antituberculous agents were used together with antibiotics. Because the NTM PCR test was positive on the fourth hospital day, antituberculous agents were discontinued, and treatment was continued with amikacin (250 mg every 24 h), cefoxitin (3 g every 24 h), and clarithromycin (375 mg every 24 h). M. chelonae was confirmed in the NTM culture, and antimicrobial susceptibility testing results were as shown in Table 3. Appropriate use of antibiotics was maintained, but as the wound did not improve, amputation was performed below the left knee after 4 weeks. Amikacin and cefoxitin were discontinued after being used for 2 weeks, and rifabutin (150 mg every 24 h) was used for 3 weeks. Treatment was maintained with clarithromycin (375 mg every 12 h), but the patient died from an aggravated systemic illness.
Discussion
The data collected in this research consisted of skin and soft tissue infections caused by RGM in Korea from 1995 to the present, and a total of 15 references were included in the review. Thus far, there have been no domestic reports of cases following prosthesis implantation aside from our cases. Regarding the area of occurrence, 21 patients had skin and subcutaneous infections, while 5 patients had soft tissue infections and osteomyelitis. The strains that caused these infections were mainly the M. fortuitum complex, M. chelonae, and M. abscessus. When compared to domestic research results, they showed similar results to Lee et al [13], who reported an incidence of 36% for M. fortuitum and 36% for M. abscessus. Providing overseas data, Hsiao et al [28] reported that M. abscessus was the most common strain in 58 patients with skin and soft tissue infections. In addition, Chen et al [29] reported a high occurrence of infection from M. fortuitum and M. marinum was reported to be associated with invasive procedures. Albert et al [30] reported that soft tissue infections occurred from M. chelonae and M. fortuitum after prosthesis implantation and successful treatment was achieved by removing the prosthetic appliance and using more than one drug for more than 6 months.
Although not included in this analysis, there have been reports of skin and soft tissue infection outbreaks. Kim et al [11] reported that 77 patients were infected with M. massiliense after intramuscular injection of ribostamycin sulfate at a local clinic, and Song et al [12] reported that 40 patients were infected with M. abscessus after receiving acupuncture. As in such reports, RGM outbreaks can be an important epidemiologic problem. When such patients are found, a connection to the outbreak should always be considered in taking the medical history.
In patients 3 and 4 at our hospital, RGM infection was confirmed 3 to 4 weeks after the implantation of a prosthetic appliance in the shoulder joint. As incision, drain, and antibiotic treatment resulted in improvements, the prosthetic appliance was not removed. This was due to the heightened rate of diagnosis achieved through tissue biopsy testing together with PCR, which are used in order to obtain suitable specimens and achieve early administration of antibiotics with susceptibility. Albert et al [30] reported that 3 out of 8 patients with RGM infections were treated with combination antimicrobial therapy.
Over the last 10 years, there have been 6 cases of skin and soft tissue infections from NTM at our hospital, and the 5 patient reports in this paper occurred within the last 6 months. Therefore, the authors became interested in the connection between NTM and climate change. According to data from the National Institute of Metrological Research, the annual mean temperature and rainfall increased 1.6℃ and 94.4 mm over a recent 10-year period (2000-2009) on Jeju Island [31].
Unlike mycobacterium, nontuberculous mycobacteria originate in nature and characteristically grow well in places where freshwater and seawater meet, where it is warm and humid, and where the soil is acidic [32]. In 2008, Han et al [33] reported that the isolation rate of NTM for each season differs according to the changes in temperature and rainfall; thus, there is a need for more research regarding the interconnected relationships between climate change in Jeju and diseases caused by NTM.
In the cases experienced by the authors, 4 patients (patient 2-5) had a past history of frequent exposure to the public bath or exposure within 2-3 weeks of symptoms. As these public baths were in different areas, it was impossible to collect the water from them at the time of the patients' exposures. Thus, it is difficult to conclude that there is a correlation. When there is an outbreak, however, practitioners should consider conducting an epidemiological study and investing the time and resources necessary to collect specimens from the surrounding environment, as well as confirm whether cases are identical through PCR and culture studies.
Since Korea has a higher incidence of tuberculosis than other countries, Korean medical practitioners tend primarily to use antituberculous therapy when the AFB stain is positive although the PCR test is negative. In addition, if the suspected infection produces a low colony or if the PCR test is negative, the prevalence of tuberculosis and lack of knowledge regarding NTM can lead to a missed opportunity for treatment. Therefore, although it is not possible to test for NTM in all patients, it is advisable to refer to these analysis results and conduct PCR tests and culture studies for NTM in cases where the patients are elderly and female, have an operation history, have had exposure to water, and have suffered from wounds with delayed recovery. There is also a need to check antimicrobial susceptibility testing results.
The limitations of this paper are as follows: first, insufficient data on domestic cases was collected for retrospective analysis. Second, several of the cases lacked medical histories and antimicrobial susceptibility testing. Until now, however, there has been a lack of analysis regarding RGM in Korea, and such cases have been treated initially as general wound infections. As a result, it is difficult to conduct a prospective study. Under such restricted conditions, the analysis of cases to the present may be used as background for future analyses.
The recent increase in the frequency of NTM infections has attracted increased attention from clinicians, but there is still a lack of awareness. When infections occur after operations, NTM infections should be suspected along with usual post operative wound infection, and active diagnostic efforts are required using special stains, cultures, antimicrobial susceptibility testing, and PCR. In our data analysis, M. fortuitum was the most common strain among skin and soft tissue infections caused by RGM in Korea. There were cases in which it obtained inducible resistance to clarithromycin, which is used as a primary medication. Hence, it is necessary to identify the correct strain as well as examine antimicrobial susceptibility testing results before beginning treatment.




 XML Download
XML Download