

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Bloodstream infection (BSI) is an important cause of morbidity and mortality in severely immunocompromised patients with hematologic malignancies undergoing chemotherapy (CTx) or stem cell transplantation (SCT) [1]. Also, BSI can result in delays in CTx, extension of admission period, and increased costs of antimicrobial therapy against target organisms [2]. The causative organisms of BSI have changed over time due to the wide use of long-term central venous catheters such as a Hickman catheter, use of prophylactic antibiotics, administration of initial empirical broad-spectrum antibiotics for neutropenic fever, changes in empirical antifungal therapy, improvement in adjuvant therapies using transfusion and G-CSF, and increased awareness of the importance of infection control [3-5].
The frequency of gram-positive bacteria (GPB) as a microbial cause of BSI has continuously increased in U.S. or Europe, but in Asia, it has been reported until recently that the frequency of BSI caused by gram-negative bacteria (GNB) was high regardless of presence of neutropenia, and the resistant pattern of isolated organisms against antibiotics have changed over time [3, 6-8]. Therefore, due to such differences in the distribution of causative microorganisms and antibiotic resistance, empirical antibiotics should be carefully selected considering the characteristics of each region and hospital rather than uniformly applying published guidelines without careful consideration.
The Catholic Blood and Marrow Transplantation (BMT) center moved to a new hospital in April, 2009. This study investigated epidemiological and clinical features of BSI that were observed in two different hematology wards which provided different treatments and compared different aspects of BSI between the two wards for the period of one year after moving to a new hospital.
Materials and Methods
1. Data collection
We retrospectively reviewed medical data of all consecutive patients over 15 years old who had been hospitalized and received CTx or SCT in the hematology wards at the Catholic University Seoul St. Mary's Hospital, the Catholic BMT center over the period of 1 year, from June, 2009 through May, 2010. Among all consecutive patients over, those who showed signs or symptoms of infectious diseases and had positive blood cultures were targeted.
As of May 2010, the hematology wards where patients of hematologic malignancies are hospitalized and receive CTx (ward A) or SCT (ward B) were separated from other wards and managed under special infection control guidelines. Ward A was mainly used to perform high-dose CTx for acute leukemia and malignant lymphoma, collect peripheral stem cells for autologous SCT, or administer antithymocyte globulin to aplastic anemia patients; ward B was mostly for the patients treated with autologous or allogenic SCT.
We collected two sets of blood samples from each patient; each set consisted of a sample from central venous catheter sample and peripheral vein puncture, for a total of 10-12 mL. Two sets of blood samples were obtained from two different peripheral veins when a central venous catheter was absent. A blood volume of 5-6 mL of each set was injected into each aerobic and anaerobic blood culture bottles (BD Bactec Plus Aerobic/F, Lytic/10 Anaerobic/F Culture Vials, Becton Dickinson and Company, Sparks, MD, USA) and immediately transported to a laboratory. The Bactec FX (bioMerieux inc., Durham, NC, USA) blood culture medium was used, and then subcultures were made on the blood agar medium and MacConkey medium when bacteria was cultured within 5 days. Antibiotic susceptibility tests were performed using automated systems (Vitek-2, bioMerieux Inc., Hazelwood, MO, USA). The clinical data were collected from reviewing medical records of each patient with bacteremia, which were age, sex, diagnosis, type of therapy, absolute neutrophil counts, C-reactive protein (CRP), Pitt bacteremia score, presence of central venous catheter, identification of bacteria and antibiotic susceptibility tests, clinical courses, and other clinical information during the BSI.
2. Definitions
Fever was defined as an increase in body temperature to over ≥38.0℃ using a tympanic thermometer. Neutropenia was defined as an absolute neutrophil count of <500 cells/mm3 or a count of <1,000 cells/mm3 with a predicted decrease to <500 cells/mm3 within the next 2 days [7].
Bacteremia was defined as an isolation of organisms from at least one blood culture bottles. If the bloodstream isolate was a potential skin contaminant (e.g. diphtheroids, Propionibacterium species, Bacillus species, coagulase negative staphylococci, or Micrococci), it was considered a true pathogen when antibiotic treatment was started and the patient had compatible clinical signs and symptom [4]. BSI was considered polymicrobial if 2 or more pathogens were isolated in a single blood culture at the same time or in separate blood cultures obtained within 48 hours apart [9]. Bacteremia occurring more than 14 days after a previous episode and separated by repeatedly negative blood cultures was considered to be a separate BSI [9]. Subsequent isolation of the same pathogen within 14 days was considered a persistent bacteremia. Pathogens with intermediate susceptibility or resistance were considered resistant. A BSI was defined as bacteremia or fungemia.
3. Initial empirical antibiotics and prophylaxis
The Catholic BMT center prescribed anti-pseudomonal cephalosporins (ceftazidime or cefepime 2 g q 12hr IV) and aminoglycoside (isepamicin 400 mg q 24hr IV) combination therapy as initial empirical antibiotics when neutropenic fever occurred during the study period. Prophylactic antibiotics were administered as follows: ciprofloxacin (500 mg q 12hr PO) and fluconazole (100 mg q 24hr PO) were given to patients with acute leukemia treated with CTx from the beginning during the neutropenic period, whereas ciprofloxacin and itraconazole syrup (200 mg q 12hr PO), or micafungin (50 mg q 24hr IV)were administered to patients treated with SCT from the early stage of administration of conditioning regimens until neutropenia was resolved. Statistical significance was defined as a two tailed P-value <0.05.
4. Statistics
Descriptive statistics were expressed as mean standard deviation for continuous variables, and ratio or percentage for categorical variables. Statistical significance was assessed via the Chi-square test or the Fisher exact test for categorical variables, and the Student t-test or the Mann-Whitney U-test for continuous variables. Log-linear model was used to compare the incidence rate of BSIs between 2 hematology wards. Survival rate was estimated by using the Kaplan-Meier method and curves were compared with use of the log-rank test. Statistical analysis was performed using SPSS ver. 12.0 (SPSS Korea, Seoul, Korea).
Results
1. Characteristics of the patients
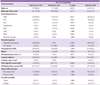
Clinical characteristics of all patients hospitalized in ward A or B during the study period were described in Table 1. A total of 488 patients were hospitalized 851 times; of them 56.4% were men and the mean age (SD) was 43.5 (13.5) years. Patients with acute leukemia accounted for more than 70%, followed by multiple myeloma (7.1%) and aplastic anemia (6.2%). Patients were treated mostly with CTx in ward A and SCT in ward B with a mean admission days (SD) of 26.7 (10.8).
A total of 159 patients developed BSI with 198 times of hospitalization. Fifteen patients experienced monomicrobial BSI twice or more during one hospitalization, and 2 of them experienced monomicrobial BSI three times in total. One patient experienced two episodes of polymicrobial BSI and the other had one episode of each monomicrobial BSI and polymicrobial BSI during the same period of hospitalization.
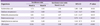
A total of 222 episodes of BSI including 20 episodes of polymicrobial bacteremia were detected, 220 episodes were bacteremia and 2 episodes were fungemia. Men accounted for 51.4% with the mean age (SD) of 44.6 (13.5) years old. In regard with underlying diseases, acute myelogenous leukemia was most commonly found in 136 (61.2%) patients, followed by aplastic anemia in 8 (3.6%) patients, and malignant lymphoma in 6 (2.7%) patients (Table 2). BSI occurred in 2 patients receiving SCT in ward A and these patients had been transferred to continue the treatment in ward A until gaining stable general condition after recovering from neutropenia with treatment with SCT in ward B.
When comparing differences in underlying diseases detected between the two wards, acute myelogenous leukemia were more frequent in ward A whereas aplastic anemia and multiple myeloma were more frequent in ward B (Table 2). There was not much difference between two wards in regard with sex, age, presence of neutropenia at BSI, Pitt bacteremia score, presence of central venous catheter, C-reactive protein, admission days, type of BSI, and overall mortality at 7 and 30 days.
Except for 1 (0.5%) episode, a total of 221 (99.5%) episodes had indwelling central venous catheters, and the Hickman catheter was the most common type used in 208 (93.7%) cases, followed by chemoport in 8 (3.6%) cases, short-term central venous catheter in 4 (1.8%) cases, and hemodialysis catheter in 1 (0.5%) case. The frequency of BSI per 1,000 catheter-days in ward A and B was 10.2 and 4.7 episodes, respectively with 8.8 episodes per 1,000 catheter-days in total. In 14 episodes, a catheter was removed within 2 weeks after BSI had developed.
2. Distribution of microorganisms and incidence of BSI
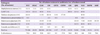
Of the 20 episodes of polymicrobial BSI, 3 bacteria were isolated in 1 episode and 2 bacteria isolated in 19 episodes, which made a total of 243 bacterial strains isolated (Table 3). The strains consisted of 122 Gram-positive bacterial strains (50.2%), 119 Gram-negative bacterial stains (49.0%), and 2 fungal strains (0.8%). Escherichi. coli was the most prevalent isolated organism, accounting for 72 strains (29.6%) followed by viridans streptococci (n=44, 18.1%), Enterococcus species (n=34, 14.0%), and Klebsiella pneumoniae (n=31, 12.8%). All 2 episodes of fungemia occurred in ward A, and the frequency of E. coli tended to be higher in ward A (42.4%) than that (27.6%) in ward B, yet significant difference was not observed. In addition, there was no difference observed in the distribution of other organisms in the two wards. However, in the comparison of monomicrobial bacteremia and all bacteria isolated in polymicrobial bacteremia episodes, the frequency of Enterococcus species in polymicrobial bacteremia was higher than monomicrobial bacteremia (P<0.001).
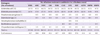
Total incidence of BSI per 1,000 patient-days in the entire ward was 9.76 episodes for one year, with 12.33 episodes in ward A and 4.28 episodes in ward B, which made incidence of ward A significantly higher than that of ward B (incidence ratio ward A vs. B 2.88, 95% confidence interval [CI] 1.97-4.22, P<0.001). Among 5 most frequently isolated organisms, the incidences of E. coli, viridans streptococci, and Klebsiella pneumoniae in ward A were significantly higher than those in ward B, and the incidences of Enterococcus species and Staphylococcus aureus in ward A tended to be higher than those in ward B, yet no statistical significance was observed (Table 4).
The bacteria isolated from the sites that had shown signs of infection in 16 patients were concordant with those cultured from blood (Table 5). The number of infection sites consisted of 7 cases of skin and soft tissue infections including superinfections, 5 cases of catheter, 3 cases of urinary tract and 2 cases of lung.
3. Antibiotic susceptibility of isolated microorganisms
Results of antibiotic susceptibility of GPB and GNB are described in table 6 and 7 each. The resistance rate of GPB against each antibiotic was 70.8% for penicillin, 55.8% for clindamycin, 62.5% for erythromycin, and 85.2% for quionolone. The resistance rate of S. aureus against oxacicllin was 63.6%. Among Enterococcus species, all E. faecium strains were resistant to ampicillin, and the resistance to vancomycin was found in 36.8% of E. faecium, but not in E. faecalis strains. The resistance rate of GNB against each of the following antibiotics was: amikacin 10.6%; levofloxacin 82.5%; trimethoprim/sulfamethoxazole 57.6%; and imipenem 4.4%. The most common isolated microorganism was E. coli (34.9%), and 71.0% of K. pneumoniae were extended spectrum beta-lactamase (ESBL)-producing strains. All Stenotrophomonas maltophilia isolates were found to be susceptible to both levofloxacin and trimethoprim/sulfamethoxazole. One strain was isolated from Chryseobacterium indologenes, and only this strain was resistant to meropenem among all isolated strains.
4. Fungemia and prophylactic antifungals
Two episodes of fungemia occurred in ward A, and Candida tropicalis and Trichosporon asahii were isolated from each episode. The first case of fungemia was detected while the patient was receiving induction remission CTx for acute myelogenous leukemia and fluconazole as a prophylactic, and the patient survived for more than a month after recovering from fungemia. The second one was detected while the patient was receiving induction remission CTx for acute lymphoblastic leukemia and itraconazole syrup as a prophylactic, and the patient died from renal failure before the fungus was isolated. Of prophylactic antifungal agents administered to all 222 episodes of BSI, fluconazole was most frequently administered to 116 cases (52.2%) followed by itraconazole to 74 cases (33.3%), micafungin to 16 cases (7.2%), and voriconazole to 5 cases (2.3%), and 10 cases (4.5%) did not receive any prophylactic antifungal agents.
5. Prognosis
The mortality rate for 7 and 30 days after BSI occurred was respectively 4.7% and 3.2% in ward A and 14.1% and 6.5% in ward B, yet no significant difference was observed. Univariate analysis was performed to assess survival rate associated with sex, presence of neutropenia, polymicrobial bacteremia, presence of ESBL, Pitt bacteremia score, and results of blood isolates (positive vs. negative), but no significant difference was found. In addition, mortality rate in the case of shock was higher than that without shock (P<0.001).
Discussion
This study investigated epidemiology of BSI which had occurred in the two hematology wards over 1 year. The total incidence of BSI was 9.76 episodes per 1,000 patient-days, and the BSI incidence (12.33 episodes) of ward A where CTx was mostly performed was significantly higher than that (4.28 episodes) of ward B where SCT was mostly performed. Previous studies of the epidemiology of BSI mostly targeted patients with BSI and reported the types of organisms isolated and their resistance patterns [6, 9-11]. This study evaluated the BSI incidences of all hospitalized patients during the study period, with consideration for their hospital stay as well as investigation on clinical characteristics of patients with BSI. The incidence of BSI could be calculated by inferring from the number of all hospitalized patients or infected in several previous studies [9, 11-13]. Choi et al. analyzed patients receiving induction remission CTx out of acute leukemia patients and reported 47 episodes of primary bacteremia (14.4%) during a total of 326 cases of CTx [13], and Oliveira et al. reported 91 patients with bacteremia (22.1%) out of 411 patients treated with SCT [11]. The study by Choi et al. targeted only acute leukemia patients who received induction remission CTx and showed information only about primary bacteremia, and therefore it may be inappropriate to compare the study with ours. Of the 253 SCT patients hospitalized in ward B, 31 patients (12.3%) developed bacteremia, and the incidence was lower than that of the study by Oliveira et al. However, several differences were observed in the study of Oliveira et al. compared with this study: chronic myelogenous leukemia was found to be the most common underlying disease (n=75, 33%); their study subjects included those of intensive care units as well as general wards; and follow-up was undertaken until the time of recovering from neutropenia or death.
Overall, the isolation ratio between GPB and GNB from blood was similar (50.6% vs. 49.4%), and no difference was observed in the causative organisms between the two wards. According to the study on the infection pattern of patients with acute leukemia from 1988 to 1995, GNB were isolated more frequently than GPB in microbiologically documented infections (63% vs. 27.5%), yet in comparison of the infection patterns in 1980s [14], the ratio of GNB showed gradual increase whereas the ratio of GPB became less. Yet, no significant difference between GNB and GPB was found, and neither was in our study. Previous studies investigated all microbiologically documented infections including BSI, and BSI accounted for 20-30% of all infections. In the past, GNB was mainly associated with causing BSI in malignant tumor patients with neutropenia, but recently it became more towards GPB [4-5, 15-19]. However, such trend is different depending on regions, and many studies still recognized GNB as main causative agents [10, 20-22]. Wisplinghoff et al. published a study on the causative agent of BSI in cancer patients, including those with hematologic malignancies, in the United States for six years from 1995 to 2001 [4] and observed a significant increase in the GPB ratio consisting of all BSIs (62% vs. 76%, P<0.001). In their study, the ratio of patients with neutropenia was 29.4% (n=798), in which GPB accounted for 61% with the highest ratio of coagulase negative staphylococci (CoNS, 31.6%) and GNB 24.9%, with E. coli accounting for the highest ratio (7.3%). Wang et al. investigated bacteremia in patients with hematologic disease in one tertiary hospital in Taiwan during two separate periods, 1995-1996 and 1999-2002, and reported that GNB accounted for more than 70% in both periods, which generated different results from other studies done in US and Europe [10, 21]. In our study, E. coli accounted for the highest ratio; however, in contradiction with the findings of Wang et al., the ratio of each GPB and GNB were similar and instead of S. aureus, the viridians streptococci accounted for the highest ratio among GPB. Wang et al. did not use prophylactic antibiotics during the study period, in contradiction with our study in which ciprofloxacin was used as a prophylactic, and such differences in prophylactic antibiotic regimen and strength or types of CTx might affect distribution of causative organisms in BSI [2, 10].
Increase in the resistance rate of GNB is known to be associated with the use of prophylactic antibiotics [2], and differences in the resistance rate depending on the use of prophylactic antibiotics were observed in several studies [6, 9, 10, 22]. In Mikulska et al.'s study that used ciprofloxacin prophylactic regimen, the resistance rate of E. coli and K. pneumoniae against quinolone (91%) and ESBL producing rate (41%) were consistent with our study [9]. The resistance rate of Pseudomonas species against carbapenem was greatly different depending on studies ranging from 6% to 91% [4, 6, 9, 10, 22], and in this study, 4 strains out of 5 were resistant to imipenem. Over the study period, our hospital provided a combination of cephalosporins and aminoglycoside effective against Pseudomonas species as initial empirical antibiotics to those with neutropenic fever [12]. In cases that did not respond to antibiotics after 3-5 days, an empirical antifungal agent was added, and we considered changing the initial antibacterial drugs to the carbapenem. In this study, the resistance rate of isolated GNB against ceftazidime was high (43.9%), yet the resistance rate to amikacin was around 10%; therefore it could be evidence for the administration of an initial combination regimen. In addition, considering that carbapenem-resistant enterobacteriaceae (CRE) infection has increased recently [23-25], the strategy of not administering carbapenem-type antibiotics from the beginning of BSIs may be desirable for the control of CRE.
The second most prevalent bacteria isolated was viridans streptococci (n=44, 18.1%), and since it was first detected in the blood culture of cancer patients with neutropenia in 1978, this bacteria have been recognized as main causative organisms for bacteremia in those, including cancer patients, with severe neutropenia, severe oral mucositis patients, and patients treated with high-dose cytosine arabinoside [26-29]. The resistance rate of viridans streptococci against penicillin was reported variously from 14% up to 64% [4, 6, 10, 29]. Regarding other GPB, CoNS showed resistance to oxacillin in most previous studies, which is consistent with results of our study, and the resistance rate of S. aureus against oxacillin was reported over 50% in recent studies, despite the differences depending on studies [6, 9, 10]. In this study, the resistance rate of E. faecium against vancomycin was 36.8%, which was lower than that reported in the US [4, 30], but similar to that reported in Taiwan and Europe [6, 31].
Although the uniform use of glycopeptide to patients with neutropenic fever in the early stages was not recommended [32], some medical centers administered glycopeptides to patients with severe mucositis from the early stages [28]. However, the use of glycopeptides should be carefully determined due to the danger of emergence of vancomycin-resistant enterococci. Considering the high resistance rate of GPB against penicillin and oxacillin, our center added glycopeptides to initial antibiotics only when we were informed that GPB were isolated from blood culture, shock was accompanied, or there was skin and soft tissue infection or catheter associated infection, and we carefully made a determination of whether or not maintaining, changing, or suspending of glycopeptides after checking bacterial isolation and antibiotic susceptibilities.
All patients, except one, had indwelling central venous catheters, of which 93.7% were Hickman catheters. Among 15 cases from which catheters were removed, tip culture was performed in 7 cases and the same bacteria isolated from blood culture were isolated in 5 cases. We tried to keep the catheters as long as possible in patients with long-lasting neutropenia or severe thrombocytopenia, and since tip culture was not performed in all 15 patients, we are unable to determine whether or not catheter-related infections occurred. The newly published treatment guideline for patients with neutropenic fever recommended to measure differential time positivity (DTP) in order to distinguish catheter-related infections [7]. However, previous studies on DTP did not target long-term maintenance catheters such as the Hickman catheter, and therefore more careful interpretations should be made especially for the cases in which antibiotics were already administered due to the low specificity of the test [7], and further studies are needed in this area.
Only 2 episodes of fungemia occurred during the study period, accounting for 0.8% of all BSI cases. The ratio of fungemia that comprise of all BSI cases also differed in 2-10% depending on regions and time [4, 5, 8, 12]. In our center, for the prevention of fungal infection, fluconazole (100 mg q 24hr PO) during CTx for acute leukemia and itraconazole syrup (200 mg q 12hr PO) or micafungin (50 mg q 24hr IV) during SCT are administered. Further studies may be needed on the preventive effect of all fungal infection, yet current usage and dosage of a prophylactic antifungal agent seems to be effective for the prevention of fungemia at least.
There was no difference in total mortality at 7 and 30 days between the two wards, but in the univariate analysis, mortality in patients with presence of shock was found to be higher than that in patients without shock. Like other previous studies, polymicrobial bacteremia did not influence the prognosis [33, 34].
There are several limitations to this study as a retrospective chart review. First, symptoms and signs related to BSIs that actually occurred might not have been recorded. As a result, it was quite difficult to evaluate the primary focus of BSI. Second, the study was limited to understand an overall trend, because the data was collected for relatively short period of time, 1 year. Yet, the number of study subjects was not less than studies previously done [5, 20, 22], and therefore it may be helpful to grasp current situations. Third, the severity and prognosis of the entire hospitalization period of patients with BSIs may be difficult to be reflected since intensive care unit acquired BSI was not included. Despite these limitations, our study finds its significance in that it was the first incidence study of BSI conducted in Korea with consideration of admission days as well as the number of patients treated with high-dose CTx or SCT due to hematologic malignancies. Further prospective studies will be needed to understand the primary focus of BSI and association with catheters.
In conclusion, the incidence of BSI in patients treated with CTx was higher than that with SCT, but there was no difference in the distribution of bacteria isolated and prognosis. The most prevalent isolated bacteria were E. coli, followed by viridans streptococci, and K. pneumoniae. BSI in patients with hematologic malignancies can be different in the distribution of causative agents and antibiotic resistance profiles depending on regions, medical facilities, and time, and therefore the selection of individualized empirical antibiotics should be based on the current epidemiology of each region and medical facility, and resistance pattern.



 XML Download
XML Download