

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Invasive aspergillosis (IA) is a major life-threatening infection in neutropenic patients and stem cell transplantation recipients [1, 2]. Voriconazole is currently recommended as the primary antifungal therapy for IA [3]. Because voriconazole exhibits non-linear pharmacokinetics and wide intra- and inter-individual variability, therapeutic drug monitoring (TDM) may improve the efficacy and reduce the toxicity of voriconazole therapy [4-6].
Voriconazole is extensively metabolized by hepatic cytochrome P450 isoenzymes including CYP2C19, CYP2C9, and CYP3A4 [7]. Genetic polymorphisms in CYP2C19 mainly contribute to the significant variability of voriconazole pharmacokinetics [8, 9]. Several studies demonstrate that voriconazole exposure is approximately 3-4 and 2 times higher in poor metabolizers (PMs) and heterozygous extensive metabolizers (HEMs) compared to homozygous extensive metabolizers (EMs) [8, 10]. The variability in voriconazole concentrations may influence both its therapeutic efficacy and toxicity [11, 12]. However, factors besides CYP2C19 genetic polymorphisms are responsible for the pharmacokinetic variability of voriconazole, and no dose adjustment with respect to CYP2C19 genotype has been established [5, 13].
We investigated the impact of CYP2C19 genetic polymorphisms on voriconazole trough levels, treatment response, and therapeutic toxicity in Korean patients with IA treated with voriconazole under routine voriconazole TDM.
Materials and Methods
1. Study design and patients
In this prospective observational study, all patients ≥ 18 years of age who received voriconazole therapy for at least 4 days at the Catholic Blood and Marrow Transplantation Center in Korea from January 2011 to June 2012 were enrolled consecutively. Voriconazole was administered to treat probable or proven IA as defined by the European Organization for the Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group as well as the National Institute of Allergy and Infectious Diseases Mycoses Study Group Consensus Group [14]. The administration route and dosage of initial voriconazole therapy were determined by the investigators on the basis of the manufacturer's recommendations and the following published guidelines [3]: 6 mg/kg intravenous voriconazole twice on the first day followed by 4 mg/kg twice daily or 200 mg oral voriconazole twice daily. For patients with moderate or severe renal impairment (i.e., estimated creatinine clearance using the Cockroft.Gault equation < 50 mL/min) at baseline, oral formulations were preferred over intravenous administration. The following data were collected for each patient: basic demographic data, underlying hematological disease, IA clinical characteristics, concomitant medications during voriconazole therapy, CYP2C19 genotype, voriconazole trough levels, response to voriconazole therapy, and adverse events during the study period. Voriconazole therapy was continued for a minimum of 6 weeks or until the lesions resolved, unless breakthrough invasive fungal infections (IFIs), voriconazole-related serious adverse events (SAEs), or death occurred. This study was approved by the Institutional Review Board of Seoul St. Mary's Hospital (KC12RISI0518).
2. Voriconazole therapeutic drug monitoring and CYP2C19 genotyping
Serum voriconazole trough levels were measured by high-performance liquid chromatography (HPLC) coupled to tandem mass spectrometry as described previously [15]. Chromatography was performed on a Waters Alliance® 2795 HT HPLC system (Waters Corporation, Milford, MA, USA). First blood sampling was done at least 4 days after starting therapy right before the next voriconazole dose. The target range for voriconazole trough levels was 1-5.5 mg/L [4, 5, 16, 17]. TDM was repeated on the fourth day if there was any change in voriconazole dosage or administration route, or when voriconazole-related toxicities or a lack of response was suspected. Voriconazole dosage was increased or decreased 25-100% in patients who exhibited out-of-range trough levels on the basis of clinical judgment by infectious diseases specialists.
DNA was extracted from buccal swab for CYP2C19 genotyping. CYP2C19 genetic polymorphisms were determined using a Seeplex® CYP2C19 ACE Genotyping system (Seegene, Seoul, Korea) according to the manufacturer's instructions; this system is a multiplex polymerase chain reaction system for detecting the CYP2C19*2 and CYP2C19*3 alleles. The CYP2C19*17 allele was determined using polymerase chain reaction-restriction fragment length polymorphism analysis as described previously [18] and sequencing. CYP2C19 phenotypic subgroups were classified as follows: EMs, carriers of 2 wild-type alleles (CYP2C19*1) or 1 wild-type allele and 1 CYP2C19*17; HEMs, carriers of 1 null allele and 1 wild-type allele; and PMs, carriers of 2 null alleles (most commonly CYP2C19*2 or CYP2C19*3) [19, 20].
3. Definitions
Treatment response was determined 12 weeks after the start of voriconazole therapy on the basis of clinical, radiological, and mycological data according to the previously established consensus criteria [21]: success (i.e., complete or partial response) or failure (i.e., stable response, disease progression, or death during the study period regardless of cause). A breakthrough IFI was defined as occurring > 6 days after the initiation of voriconazole therapy or < 6 days after the discontinuation of voriconazole therapy [22]. The discontinuation of voriconazole due to breakthrough IFI development or voriconazole-related adverse events were also regarded as treatment failure. Deaths were attributed to IA unless there was an apparent primary cause of death unrelated to IA.
All AEs that occurred during voriconazole therapy or up to 72 h after treatment were recorded regardless of whether they were causally related to voriconazole. The category and grade of AEs were defined according to the National Cancer Institute [23]. Grades 3-5 were considered SAEs. The causal relationships between adverse events and voriconazole therapy were assessed using the Naranjo Probability Scale [24]. Finally, definite, probable, or possible AEs were included in the analysis.
4. Statistical analysis
Continuous variables are expressed as mean [standard deviation (SD)] or median [interquartile range (IQR)]. The Chi-square test or Fisher's exact test was used to compare categorical variables. Meanwhile, Student's t-test or the Mann-Whitney U-test was used to compare continuous variables. One-way analysis of variance with post hoc tests (i.e., Games-Howell) or the Kruskal.Wallis test was applied to test for differences in voriconazole trough levels among the 3 CYP2C19 genotypes. Two-sided P-values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
Results
1. Patient characteristics
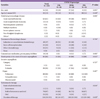
A total of 104 patients were consecutively enrolled in this study. Their demographic and clinical characteristics are summarized in Table 1. Their mean (SD) age was 53 (13) years, and 54 (52%) patients were male. Acute leukemia (73%) including acute myeloid and lymphoblastic leukemia was the most frequent hematologic disease. Concomitant use of proton pump inhibitors was recorded in 10 patients. There were no significant differences among CYP2C19 genotypes with respect to age, sex, hematologic disease characteristics, concomitant medications, IA, or voriconazole therapy.
2. CYP2C19 genotype and TDM
The wild-type allele CYP2C19*1 was observed most frequently (126/208, 61%) followed by CYP2C19*2 (53/208, 25%), CYP2C19*3 (27/208, 13%), and CYP2C19*17 (2/208, 1%). There were 37 (36%), 2 (2%), 32 (31%), 18 (17%), 6 (6%), and 9 (9%) patients with CYP2C19*1/*1, *1/*17, *1/*2, *1/*3, *2/*2, and *3/*3 genotypes, respectively. The distribution of CYP2C19 genotypes was 39 (38%), 50 (48%), and 15 (14%) EMs, HEMs, and PMs, respectively.
A total of 511 voriconazole trough levels from 104 patients were measured. A median of 3 (IQR, 2-7) samples for TDM per patient were analyzed. The median time from starting voriconazole therapy to the measurement of initial trough level was 6 days (IQR, 4-7 days). Overall, the median (IQR) initial trough level was 2.5 (1.28-4.13) mg/L. The initial trough levels in 2 patients with heterozygous CYP2C19*1/*17 were 2.3 and 3.0 mg/L, respectively. Fig. 1 shows the median (IQR) initial trough level according to CYP2C19 genotype: 1.8 (0.8-3.6), 2.7 (1.5-4.6), and 3.2 (2.2-3.7) mg/L in EMs, HEMs, and PMs, respectively. There was no significant difference in the initial trough levels among the 3 groups (P = 0.068). The differences between each group were as follows: P = 0.043 between EMs and HEMs, P = 0.062 between EMs and PMs, and P = 0.779 between HEMs and PMs.
The initial trough levels were outside of the target range in 31 of 104 patients (30%); among them, 19 (18%) and 12 (12%) patients were below and above the target range, respectively. The percentages of patients with an out-of-range initial trough level differed significantly among the 3 groups (46% in EMs vs. 26% in HEMs vs. 0% in PMs; P = 0.001; Fig. 2A). Below-range levels were most frequently observed in EMs (33%) followed by HEMs (12%) and PMs (0%) (P = 0.005). There was no significant difference in the frequency of above-range levels among the 3 groups (13% in EMs vs. 14% in HEMs vs. 0% in PMs; P = 0.373).
Overall, 69 patients (66%) exhibited at least one out-of-range trough level during voriconazole therapy. Fig. 2B shows the incidences of out-of-range overall trough levels according to CYP2C19 genotype. The overall incidence of out-of-range trough levels was highest in EMs (77%) followed by HEMs (66%) and PMs (40%) (P = 0.037). The incidences of both below-range (64% in EMs vs. 46% in HEMs vs. 33% in PMs) and above-range levels (28% in EMs vs. 40% in HEMs vs. 20% in PMs) did not differ significantly among the 3 groups (P = 0.079 and P = 0.268, respectively).
3. Clinical outcomes and adverse events
Thirty-two patients (31%) exhibited treatment failure to voriconazole therapy. The reasons for treatment failure were death (22/104, 21%), breakthrough fungal infections (7/104, 7%), and discontinuation of voriconazole because of voriconazole-related SAEs (3/104, 3%). Breakthrough fungal infections involved unspecified invasive fungal pneumonia, invasive pulmonary aspergillosis, disseminated aspergillosis, and rhinocerebral mucormycosis in 4, 1, 1, and 1 case, respectively. The all-cause and attributable mortality rates at 12 weeks were 21% (22/104) and 10% (10/104), respectively. Table 2 shows treatment failure, and all-cause and attributable mortality at 12 weeks according to CYP2C19 genotype; there were no significant differences within or among the 3 groups.
The overall incidence of AEs was 34% (35/104). The most common category of AEs according to the organ system affected was hepatobiliary (32/104, 31%) followed by gastrointestinal (12/104, 12%), ophthalmic (7/104, 7%), neurologic (6/104, 6%), rash (4/104, 4%), and cardiovascular (1/104, 1%). SAEs developed in 25 patients (24%). There was no significant difference in the development of AEs or SAEs among groups (Table 3).
Discussion
CYP2C19 genetic polymorphisms are well known to result in various rates of voriconazole metabolism. However, the role of individual CYP2C19 genotyping in clinical practice remains to be determined. In this study, we evaluated the impact of CYP2C19 genotype on the clinical efficacy and toxicity of voriconazole in Korean patients with IA. An initial trough level < 1 mg/L was significantly more frequent in the EMs group than the other groups, and there were no patients with an out-of-range initial trough level among PMs. However, under routine voriconazole TDM, there was no significant relationship between CYP2C19 genotype and the efficacy or toxicity of voriconazole.
The distribution of CYP2C19 genotypes varies among ethnic groups [7]. The frequency of PMs is reported to be higher in Asian populations than black and Caucasian populations. In this study, the incidence of PMs in Koreans was consistent with the results of previous studies, constituting approximately 14% of the population [25, 26]; only 2 patients (2%) were CYP2C19*1/*17 heterozygous. Regarding CYP2C19 polymorphisms, higher voriconazole concentrations in patients who are PMs or lower concentrations in patients who are ultrarapid metabolizers (i.e., CYP2C19*17/*17 homozygous) have attracted the most attention. On the other hand, EMs have gone relatively unnoticed. In the present study, EMs were associated with below-range initial trough levels, while all PMs had initial trough levels within the therapeutic range. The overall incidence of out-of-range trough levels also differed significantly among the 3 groups; it was highest in EMs and lowest in PMs.
A previous study assessed the relationship between CYP2C19 genotype and out-of-range of voriconazole trough level [12]. In that study, the above- and below-range levels of voriconazole were significantly more frequent in the CYP2C19*2 and CYP2C19*17 groups, respectively. However, compared to the present study, the previous study has several differences in the study population and design: (1) the subjects were Caucasian lung transplant recipients with cystic fibrosis; (2) different distribution of CYP2C19 alleles (18.8% for CYP2C19*17, no PMs) and grouping of CYP2C19 genotype (wild-type vs. CYP2C19*2 carriers vs. CYP2C19*17 carriers); (3) the therapeutic range was 1.0.2.0 mg/L; and (4) the percentages of out-of-range values during the first 42 days and not the initial trough levels were compared among CYP2C19 groups. Considering the target trough level range proposed on the basis of several published data is 1.0-5.5 mg/L, the highly limited therapeutic range of that study could have influenced their results [4, 5, 17].
Several studies demonstrate that voriconazole serum concentrations are related to both efficacy and toxicity [4, 16, 27, 28]. Although CYP2C19 polymorphism has been identified as a major factor for voriconazole metabolism, the clinical implications of CYP2C19 polymorphisms are controversial [12, 20, 29, 30]. The observed differences in both efficacy and toxicity could be due to much more complicated situations in patients, such as genetic polymorphisms in drug-metabolizing enzymes besides CYP2C19, drug.drug interactions, comorbidities, and variations in patients' conditions such as mucositis.
In the present study, there were no differences in either efficacy or toxicity with respect to CYP2C19 genotype, although the frequency of out-of-range initial trough levels differed significantly among the 3 groups. The availability of TDM and dose adjustments based on TDM results might be responsible for these findings. A recent randomized controlled study evaluated the utility of routine TDM in patients with voriconazole therapy [6]; the results demonstrate that routine TDM of voriconazole significantly reduces the incidence of voriconazole discontinuation due to AEs and improves treatment response.
The present study has several limitations. First, only Korean patients at a single center were enrolled. Therefore, caution should be taken when applying the results to other ethnic populations. Second, the present study included relatively few patients for each CYP2C19 genotype, compromising the statistical powers of the analysis. Third, the rate of dose adjustments of voriconazole was not fixed but was rather decided on a case-by-case basis. Fourth, the results might have been influenced by previous antifungal therapy, because voriconazole was administered to all patients as second-line antifungal therapy. However, to the best of our knowledge, this is the first report on the clinical implications of CYP2C19 genotype on the efficacy and toxicity of voriconazole in Korean patients with IA.
In conclusion, there was a significant difference in the percentages of out-of-range voriconazole trough levels in both the initial and overall results among the 3 CYP2C19 genotypes; out-of-range voriconazole trough levels were highest in EMs and lowest in PMs. Below-range initial trough levels were observed most frequently in EMs, whereas there were no above-range initial trough levels among PMs. However, under routine TDM of voriconazole, the present study does not demonstrate a significant relationship between CYP2C19 genotype and either the clinical outcome or the toxicity of voriconazole in patients with IA. The clinical impact of CYP2C19 genotype might be offset by routine TDM and dose adjustments adjustments of voriconazole. From all these results indicate that increasing the loading dose of voriconazole in EMs through CYP2C19 genotyping could be considered in combination with careful TDM of voriconazole. However, further large-scale multicenter studies using clinical data from homogeneous
populations are required to confirm these results.




 XML Download
XML Download