

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Liver transplantation (LT) is a life-saving treatment for end stage liver disease. Despite improved graft survival owing to recent advances in perioperative management and surgical techniques, mortality and morbidity rates associated with perioperative infection in LT recipients remain relatively high [1-3]. Bloodstream infection (BSI) is the most frequent infectious complication, with an incidence range of 24-49%; BSI is a significant predictor of post-transplant death [2, 4-6]. Some studies have suggested that gram-positive (GP) cocci are the major pathogens of post-transplant BSI. However, others have implicated gram-negative (GN) bacilli as the predominant pathogens. Furthermore, multi-drug resistance (MDR) rates among GN bacilli have been increasing, further affecting the prognosis of LT recipients [4, 7-11].
Understanding the epidemiology of and the risk factors associated with post-transplant BSI may facilitate identification of high-risk patients, guide appropriate initiation of antibiotic therapy, and improve infection control practices. In this retrospective analysis, 222 consecutive patients who underwent LT were studied to assess the epidemiology and clinical significance of BSI in the year following LT.
Materials and Methods
1. Patient enrollment
Over a 6-year period from February 2005 to May 2011, 231 LT were performed in 222 patients at Ajou University Hospital, a university-affiliated, 1,087-bed tertiary-care institute in Korea. We retrospectively reviewed the medical records of these 222 liver transplant recipients. Deceased donor LT has been performed at this institute since 1995 and adult living donor LT since 2005. ABO-incompatible LT began in March 2007, and 11 ABO-incompatible LTs were performed during the study period [11].
2. Cultures
Microbiological surveillance cultures were routinely done after LT. Blood cultures were obtained by standard procedures and processed by an automated system. The automats used were the BacT/ALERT 3D system (bioMérieux, Durham, NC, USA) and the BACTEC FX system (BD Diagnostic Systems, USA) for rapid microbial detection. Antimicrobial susceptibility was determined by the minimal inhibitory concentration agar dilution method according to the recommendations of the Clinical and Laboratory Standards Institute.
3. Antimicrobial prophylaxis
Initial antimicrobial prophylaxis was cefoperazone/sulbactam until January 2007 and piperacillin/tazobactam subsequently. Vancomycin was routinely administered to prevent methicillin-resistant staphylococcal infections. For fungal prophylaxis, amphotericin B deoxycholate was used until December 2009, but it was replaced by liposomal amphotericin B in January 2010. The above antimicrobial regimen continued for approximately 5-7 days after LT. Intravenous ganciclovir followed by oral acyclovir or oral valacyclovir was used for cytomegalovirus prophylaxis. Pneumocystis pneumonia prophylaxis consisted of trimethoprim/sulfamethoxazole, and was continued for 1 year after LT. Selective bowel decontamination with oral neomycin was performed for recipients of elective living donor LT. Patients who received liver transplants for hepatitis B associated liver cirrhosis were managed with antiviral prophylaxis and hepatitis B immunoglobulin.
4. Immunosuppression
Primary standard immunosuppressive therapy included tacrolimus (FK506) or cyclosporine, basiliximab, and low-dose prednisone. Rejection episodes were mainly treated with high-dose methylprednisolone and by increasing tacrolimus blood concentrations.
5. Definitions
Infections were defined using the criteria proposed by the Centers for Disease Control and Prevention [12]. BSI was defined as the isolation of a pathogenic microorganism from at least 1 blood culture specimen. Skin flora organisms commonly associated with contamination were required to be isolated from 2 separate blood culture specimens. Polymicrobial BSI was defined as the isolation of > 2 organisms from a single blood culture specimen, and each organism was considered a separate isolate in the analysis. Multiple cultures that were positive for the same pathogen constituted a single BSI episode if they were not separated by > 2 weeks and the patient did not recover with negative blood culture in the interim. Pre-LT antibiotic therapy was defined as the application of broad-spectrum antibiotics for > 5 days in the month before LT. The definition of MDR bacteria was based on previous studies [13].
6. Statistical analysis
Statistical calculations were performed using the SPSS Advanced Statistics Modules, version 20.0 (SPSS, Chicago, IL, USA). Continuous data normally distributed, are expressed as mean (SD) and analyzed using the Student's t-test. All other continuous data not normally distributed are presented as median (interquartile range) and analyzed using the Mann-Whitney U-test.
The risk factors for BSI were examined by multiple logistic regression analysis. A cox regression model was used to identify independent risk factors for mortality in patients with BSI and all patients. Kaplan-Meier statistics were used to generate survival curves for patients with and without BSI. All P-values were 2-tailed, and a P-value < 0.05 was considered significant.
Results
1. Characteristics of the study population
The basic demographic and clinical characteristics of the 222 LT recipients are illustrated in Table 1. The mean age was 49 years and three-quarters of patients were men. The most frequent liver diseases leading to LT were B-viral liver cirrhosis (76.6%, 170 patients), hepatocellular carcinoma (HCC; 47.7%, 106 patients), and alcoholic liver cirrhosis (26.1%, 58 patients); ≥ 2 of these diseases overlapped in some patients. Because of the small number of other diagnoses leading to LT, only hepatitis B associated liver cirrhosis, hepatocellular carcinoma, and alcoholic liver cirrhosis were analyzed as diagnostic pretransplant variables. The study population included 33 recipients who underwent salvage LT for tumor recurrence or liver function deterioration after partial hepatectomy. Eight patients underwent a second LT for primary (n = 2) or secondary graft failure (n = 6). The median Child-Pugh score was 10 and the mean model for end stage liver disease (MELD) score was 16.
2. Time and frequency of BSI
Post-transplant BSIs occurred in 28.8% (64 of 222) of all recipients in the year after LT. A total of 135 bacterial and fungal organisms were isolated from the 112 BSI episodes including 18 polymicrobial BSIs. Thirteen patients had ≥ 1 polymicrobial BSI. One BSI occurred in 38 of 64 patients, whereas multiple episodes of BSI occurred in the remaining 26 patients, ranging from 1 to 9 episodes per patient. The median follow-up period was 1,306 (range 2-2,803) days.
Figure 1 shows the isolated time and frequency of pathogenic microorganisms in BSIs during the year after transplantation. Most of the BSIs (50.8%; 57 of 112) occurred in the first month after LT. The median time to BSI onset after LT was 28 days (dashed line) with an interquartile range (IQR) of 6-89 days; the mean time to onset was 57 ± 69 days (solid line). GP cocci, GN bacilli, and fungi were responsible for 32.8%, 52.9%, and 14.0% of isolated organisms in BSIs, respectively. The mediantime to onset of BSI episode from the date of transplantation (day 0) for each group of pathogens was day 40 (IQR: 19-113) for GP cocci (n = 44), day 23 (IQR: 6-66) for GN bacilli (n = 71), and day 12 (IQR: 5-95) for fungi (n = 19).
3. Causative pathogens and source of BSI
The distribution of species is illustrated in Table 2. Enterobacteriaceae members represented the majority of GN isolates, with the most frequent species being Klebsiella pneumoniae and Escherichia coli. Among GP organisms, Enterococcus faecium was the most common, followed by Both GP and GN pathogens showed a high rate of resistance to major antibiotics: 92.8% of S. aureus were methicillin-resistant; 38.0% of E. faecium were vancomycin-resistant; 68.4% of K. pneumoniae and 82.3% of E. coli produced extended-spectrum beta-lactamase (ESBL); and 92.8% of Acinetobacter baumannii and 91.6% of were carbapenem-resistant. However, neither linezolid-resistant enterococc or carbapenem-resistant Enterobacteriaceae were identified. Candida species accounted for 14.0% (19 of 135) of all isolates, and approximately 50% of these (10 of 19) were non-albicans species. All Candida species were susceptible to fluconazole.
The primary sources and time to onset of BSIs according to each isolated pathogen are listed in Table 3. BSIs caused by K. pneumoniae tended to occur early (median: 8 days, IQR: 4-83 days), whereas enterococcal BSIs developed later (median: 101 days, IQR: 24-153 days). The most common source was biliary tract infection (36.2%), followed by abdominal and/or wound (28.1%) and intravascular catheter (18.5%) infections. Enterococcemia or Enterobacteriaceae bacteremia from biliary tract or abdominal and/or wound infections was the most frequent type of BSI. The primary pathogens of catheter-related BSIs were Candida and A. baumannii. Polymicrobial BSIs predominantly consisted of enterococci, staphylococci, and Candida species, and most of them originated from the biliary tract.
4. Risk factors for post-transplant BSI
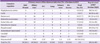
The clinical and operative variables associated with post-transplant BSI are illustrated in Table 4. Patients with BSIs were significantly more likely to have post-transplant hemodialysis, reoperative or retransplantation episodes, higher Child-Pugh score and MELD score, more transfusion during surgery, longer postoperative intensive care unit (ICU) stay and admission days, and more biliary complications. In logistic regression analysis, biliary complications (odds ratio [OR]: 2.91, 95% confidence interval [CI]: 1.29 to 6.59, P = 0.010) and longer ICU stay (OR: 1.040, 95% CI: 1.002 to 1.080, P = 0.038) were significant independent risk factors of post-transplant BSI (Table 5).
5. Survival curve and predictors for death in LT recipients
The mortality rate in LT recipients with BSI was higher than that in those without BSI in both the early (30-day mortality: 22.9% vs. 5.9%) and late (1-year mortality: 40.0% vs. 10.5%) postoperative periods. Survival time (mean ± SD) was significantly lower in patients with BSI (1,310 ± 147 days; 1-year survival rate 60.0%) than in those without BSI (2,362 ± 77 days; 1-year survival rate 89.5%) throughout the 1-year post-transplant period and beyond 1 year after LT (< 0.001) (Fig. 2).
In those with BSI, a fungal BSI was associated with the poorest 1-year survival rate (fungal BSI 35.7% vs. non-fungal BSI 66.1%). LT recipients with polymicrobial BSI also had a significantly lower 1-year survival rate than those with BSI caused by a single pathogen (polymicrobial BSI 26.7% vs. monomicrobial BSI 69.1%).
Significant predictors of mortality in the entire study population were BSI (hazard ratio [HR]: 3.92, 95% CI: 2.22 to 6.91, P < 0.001), post-transplant hemodialysis (HR: 3.38, 95% CI: 1.70 to 6.70, P < 0.001), comorbid HCC (HR: 2.14, 95% CI: 1.20 to 3.82, P = 0.009), and longer ICU stay after LT (HR: 1.024, 95% CI: 1.002 to 1.047, P = 0.030). In those patients with BSI, Candida BSI (HR: 3.71, 95% CI: 1.58 to 8.71, P = 0.003) and polymicrobial BSI (HR: 3.18, 95% CI: 1.39-7.28, P = 0.006), in particular, were independent risk factors for post-transplant death (Table 6).
Discussion
We found that BSI is a common complication for LT recipients: 28.8% of our patients developed at least 1 BSI episode inthe year following transplantation. In our study population, the rate of BSI episodes and the overall 1-year mortality rate after LT were higher than those reported by other investigators [2, 5, 14, 15]. The greater number of BSIs and the higher mortality rate in this study can be partly explained by the poor general condition of our LT recipients, whose median MELD scores (16) and Child-Pugh scores (10) were relatively high. A learning curve effect, by including in the sample those patients from the early period of our living donor LT program (a highly complex technique), might also have contributed to the increased rates of mortality and postoperative infectious complications in the early transplant period [16, 17].
Previous studies show that factors associated with post-transplant BSI include diabetes mellitus, low serum albumin level, lengthy ICU stay, reoperations, acute rejection, higher MELD score, intraoperative transfusion, biliary complication, older age, post-transplant hemodialysis, and a greater number of intravascular catheter days [2, 5, 9, 15]. In this study, biliary complication was a particularly important risk factor for BSI: 42% of LT recipients with biliary complication developed BSI. Biliary leak age or biliary stricture was a major postoperative complication, with an incidence of 10-15% in deceased donor LT and 15-30% in living donor LT [14, 18]. Biliary infections need to be studied further given the clinical significance of biliary-origin BSI in LT recipients.
BSI episodes were predominantly caused by GN bacilli, which accounted for 52.9% of all isolates. Consistent with other studies, we found that GN infections with increased MDR were common [8, 9, 15, 19, 20]. The microbial etiology of BSI varied according to the time to onset [21]. During the early period, GN bacilli including K. pneumoniae, E. coli, and A. baumannii were more frequent causes of BSIs. In the late post-transplant period, biliary-origin enterococcemia was the most frequent type of BSI. Other common BSI sources were abdominal and/or wound K. pneumoniae infection and intravascular catheter infection with Candida species or A. baumannii. It is concerning that catheter-related BSI, which is exclusively nosocomial, accounted for one-fifth of post-transplant BSIs. Further identification of BSI characteristics would aid physicians in determining the potential etiology of post-transplant BSI.
MDR pathogens accounted for the vast majority of all GN and GP bacteremia cases in this study. It was reported that resistant Acinetobacter infection has a particularly poor prognosis in LT recipients [22] and that early definite therapy seemed to influence outcomes [23]. However, therapeutic options for these organisms are often limited, expensive, and of low efficacy. Approximately one-third of enterococci showed vancomycin resistance. It is possible that our perioperative prophylaxis with vancomycin may have prevented more cases of GP BSI; however, it was not optimal in preventing infections caused by vancomycin-resistant enterococci (VRE), and may have contributed to the development of resistant organisms. Although VRE is known to be a less-virulent pathogen, VRE colonization in LT recipients has been associated with higher mortality rates regardless of the cause of death [11]. Extensive exposure to broad spectrum antibiotics in the pretransplant phase could also have influenced the increased incidence of MDR organisms. We believe that prospective studies are needed to help design strategies for the prevention of infection with these MDR pathogens and to find the optimal antibiotic prophylaxis and empirical treatment in LT.
BSI during the year after LT was the strongest predictor of post-transplant mortality, and recipients with BSI had poorer survival throughout the postoperative period than those without BSI. HCC, post-transplant hemodialysis, and prolonged ICU stay were independent risk factors for mortality in patients with BSI as well as for mortality in all patients. Many of our LT recipients had HCC (47.7%; 106 of 222 patients), and 45% of HCC cases were in an advanced stage beyond Milan criteria with a history of antitumor therapy when LT was performed. A deteriorated condition resulting from advanced cancer and the complexity of the surgery because of previous invasive therapy may have resulted in more postoperative complications and poor oncologic outcomes in these patients.
Approximately one-third of our LT recipients underwent hemodialysis after LT. It has been reported that post-transplant renal dysfunction occurs in 9-33% of LT recipients and is associated with increased mortality, especially when renal replacement therapy is required [24]. Our preoperative prophylaxis regimen included routine use of glycopeptide, amphotericin B, and ganciclovir, all of which are known to be nephrotoxic; this might have played a role in increasing the rate of post-transplant renal dysfunction. Since many LT candidates with end stage liver diseases also have marginal renal function, efforts to limit nephrotoxic medication are necessary.
BSI caused by Candida and polymicrobial BSI were significant predictors of death. One-third of candidemia cases were polymicrobial with synchronous bacteremia or other species of Candida. Candidemia and polymicrobial bacteremia may be indicators of a generally debilitated state associated with increased morbidity and mortality [25, 26]. In this study, both candidemia and polymicrobial bacteremia most frequently originated in the biliary tract or intravascular catheter. Patients with candidemia or polymicrobial bacteremia may need prompt initiation of antifungal therapy, more empirical antibacterial coverage, and active intervention such as the removal of intravascular catheters. Because of concerns over drug interactions, azole-associated hepatotoxicity, and antifungal drug resistance, amphotericin B was used for antifungal prophylaxis at our institute. However, the use of amphotericin B needs to be evaluated, given the high frequency of renal dysfunction, candidemia, and associated mortality observed in our study.
LT recipients with underlying chronic hepatitis B had better prognosis after LT in our study. United Network for Organ Sharing (UNOS) data show that, thanks to advances in antiviral therapies, recipients with hepatitis B have better post-transplant outcomes than those with hepatitis C, hepatitis B and C coinfection, and those with other liver diseases [27].
Our study has limitations because of its retrospective design, single-center study, and small sample size; therefore, our findings may not be generalizable to other institutes. BSI episodes caused by GP cocci may have been under-reported because we used strict criteria when interpreting blood culture results to rule out contaminants. The impact of BSI on post-LT mortality may also have been over-represented, since patients with BSI often had severe pre-LT status when compared with those without BSI. Because the main source of infection and the depth of infection were difficult to determine, surgical wound infections and abdominal organ/space infections were combined into a single infectious source in our study. A more sophisticated classification system should be used in future studies. Possible correlations between the antibiotics received by LT recipients and their subsequent infections including BSIs were not evaluated.
As a conclusion, Post-transplant BSI occurred at a high rate during the year after LT, particularly within the month following surgery. Patients with BSI had a significantly lower survival rate than those without BSI. GN bacilli were more frequent than GP cocci as BSI pathogens, and most of them were highly drug resistant. Biliary complication was the strongest predictor for BSI, and BSIs resulting from biliary infection were major problems for LT recipients. Prevention of BSI and biliary complication is important for improving prognosis in liver transplant recipients. BSIs caused by fungi and polymicrobial BSIs in particular were strongly associated with increased mortality. Our study provides detailed information on post-transplant BSI occurrence, and the data can be used to guide empirical antimicrobial therapy and improve infection control practices.







 XML Download
XML Download