

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The process of clinical bacteriology remains essentially unchanged from the start of the antibiotic era three-quarters of a century ago, with timings determined by the speed of bacterial growth. It takes one day to grow bacteria from the clinical specimen and another to identify them and to measure their antibiotic susceptibility. During these 48 hours the patient is treated 'empirically' or 'blind,' based on local or professional guidelines. In many instances, particularly in the community, treatment is entirely empirical, without laboratory investigation of the infection.
The only seismic acceleration has come from introduction of MALDI-TOF mass spectroscopy systems [1] (Bruker and Shimadzu/ bioMèrieux), which identify bacteria to species level within minutes starting from a pure culture (i.e. 24h after the clinical specimen). These are widely adopted in Europe, including the UK, with American licensing pending. They represent a major advance over classical identification, but do not shorten total laboratory processing time because primary culture and susceptibility testing still depend on the speed of bacterial growth [2]. Semi-automated susceptibility testing systems such as Vitek (bioMerieux) and Phoenix (BD) can deliver susceptibility results, as well as identification, in 4-10h [3, 4], reducing the total processing time to 30-34h, but this means that the final results often come in the late evening or overnight and, are often not acted upon until the following morning, obviating much of the gain. Gains in terms of mortality, morbidity, and cost are absent or extremely limited [4, 5].
More radical accelerations have been achieved by molecular methods in a few settings, notably tuberculosis and sexually-transmitted bacterial infections (STIs), but not for the generality of bacteriology. This lack of change contrasts with clinical chemistry, where near immediate results are now routine, and for virology, where there has being a seismic shift from tissue culture to molecular diagnostics [6].
Why the slowness of bacteriology matters
The slowness of bacteriology has profound implications, both for individual patients, and for antimicrobial stewardship, which seeks to extend the utility of antibiotics (Box), limiting the erosion that comes from selection of resistance.
Box: Principles of antibiotic stewardship
▪ Establish Stewardship team, involving infectious disease specialists, microbiology and pharmacy
▪ Ensure that antibiotic use guidelines are in place for common clinical settings, are appropriate to local patients, pathogens and resistance rates, and are regularly reviewed and updated
▪ Ensure, overall, that antibiotic use is proportionate to infection type and severity and is de-escalated wherever possible once microbiological data become available
▪ Audit antibiotic use guidelines, providing regular feedback and review to individual prescribers and clinical teams
▪ Balancing act between ensuring best treatment of infection in individuals vs. maintenance of antibiotic utility for society
In the community, most treatment is entirely empirical, unguided by laboratory bacteriology. In the UK, only circa 3% of community respiratory infections and circa 50% of cystitis cases have laboratory investigation and these often are the more complex cases, including those who fail to respond to primary empirical therapy owing to resistance [7]. The result is that the bacteriology laboratory investigates a biased sub-set of community specimens and over-estimates the prevalence of resistance. Since the laboratory's estimates then inform future empirical treatments, the likely consequence is that many subsequent patients are over-treated. In the UK McNulty et al [8] observed that the prevalence of trimethoprim resistance among the urinary Enterobacteriaceae routinely tested at two bacteriology laboratories was 24.5-27%, whereas this proportion halved to 14% when consecutive women presenting with uncomplicated cystitis were sampled. In other words trimethoprim remained a better treatment choice than predicted from routine data. More notoriously, resistance surveys detect high rates of penicillin nonsusceptibility in Streptococcus pneumoniae in many geographic regions yet, when consecutive respiratory patients are recruited to antibiotic trials in these locales, it proves impossible to find even a handful of patients with resistant pneumococci. If rapid bacteriological investigation could be performed at the general practitioner's office or surgery, then treatments could be better tailored to individual infections, benefitting both the patient and antibiotic stewardship.
Bacteriological investigation is more routinely performed in hospitals, at least in developed countries, but fails to recover pathogens from many patients, who nevertheless continue to receive antibiotics based upon clinical diagnosis of infection. This again leads to overtreatment, with broad-spectrum antibiotics prescribed when, in reality, the patient's symptoms derived from a non-infectious cause or when a narrow-spectrum agent could have been used if the pathogen had been identified.
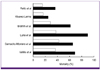
For patients with severe infection - particularly pneumonia or sepsis - a different problem arises from the slowness and imprecision of bacteriology. It is critical that these patients receive effective antibiotics within the first hour of diagnosis, since mortality increases with each hour's subsequent delay [9, 10]. If the empirical antibiotics transpire not to be appropriate against the particular pathogen there is an approximate doubling of mortality (Fig. 1) [11-16]. Inadequacy arises either because the infection involves a species inherently resistant to the antibiotic (e.g. the patient had Pseudomonas aeruginosa or methicillin-resistant Staphylococcus aureus [MRSA] but received ceftriaxone as the hospital's standard therapy for the clinical syndrome) [17] or because the particular strain of bacteria had acquired resistance (e.g. an extended-spectrum β-lactamase) [18]. The statistical hazard of inappropriate therapy grows as resistance becomes more prevalent and, in Spain, Peralta et al [19] showed a clear relationship between the numbers of resistance carried by pathogens, the frequency of inadequate treatment, and mortality.
This linkage between inadequate treatment and increased mortality been widely highlighted among critical care physicians, and leads to the empirical overtreatment of many patients, who do not have resistant pathogens, to prevent the lethal under-treatment of the few whose infections are due to these bacteria. This is understandable from an ethical standpoint but leads to poor stewardship and, in particular, to extensive empirical over-use of carbapenems, which, until recently, were reserved agents, used only for the microbiologically-directed treatment of infections due to exceptionally resistant strains. Although broad-spectrum empirical treatment should be deescalated at 48 hours, once the bacteriology data become available [20], there are many cases where the laboratory fails to grow the pathogen or where the physician is reluctant to change because the patient is responding well to treatment. Thus, Soo Hoo et al [21] found that empirical imipenem was only de-escalated, even by day 5, in around half the cases when laboratory results showed that de-escalation was possible at day 3.
As these examples illustrate, the slowness of bacteriological diagnosis increases antibiotic use and is inimical to good stewardship. This waste would matter little if we had a copious supply of new, effective antibiotics. But we do not. The numbers of antibiotics licensed has declined in each 5-year period since the early 1980s and many large pharmaceutical companies have abandoned the field, finding other areas of drug discovery more tractable or profitable [22-24]. The shortage of new antibiotics against gram-negative pathogens is especially acute, and is particularly concerning because resistance is beginning to spread even to carbapenems, with the dissemination of multiple carbapenemases particularly in Klebsiella pneumoniae [25]. These enzymes include KPC, VIM, NDM and OXA-48 types. Many producer strains are susceptible only to colistin, fosfomycin and tigecycline, none of which is suitable for widespread empirical use [26].
The slowness of bacteriology also complicates the development of new antibiotics. Patients with resistance types sought for inclusion in clinical trials cannot be identified before they have already received other antibiotics, making them ineligible for inclusion. In particular, the evaluation of narrow-spectrum antibiotics is near-impossible in life-threatening infections.
Towards a new paradigm
Advances in molecular biology provide scope to improve the speed and accuracy of diagnosing of infection and its agents [27, 28]. These developments, in turn, have the potential to radically improve stewardship, by shortening or removing the need for broad-spectrum empirical therapy. Nevertheless the barriers are considerable.
Improving diagnosis using biomarkers
Fewer patients would receive unnecessary antibiotics if it was easier to distinguish those who have bacterial infection from those whose symptoms have viral or non-infectious origins. Established indicators ('biomarkers') of infection include leukocyte counts and the estimation of C-reactive protein. These measures are sensitive, being consistently raised in bacterial infection, but have poor specificity [29]. Recent interest has centred on procalcitonin, a peptide precursor of the hormone calcitonin, which is involved in calcium homeostasis. Procalcitonin levels are raised in bacterial infections but not viral, and this can be used as a diagnostic aid, with better specificity than C-reactive protein [29, 30]. Multiple large randomised trials have been published, with >3,500 patients included, mostly with pneumonia, but also with less severe community respiratory infections [31]. Overall, the use of procalcitonin as a biomarker reduced antibiotic use and its contingent selection pressure by 30-80% without compromising clinical outcomes [31, 32]. These savings reflected both the denial of antibiotics to patients with low procalcitonin levels and briefer treatment durations in those whose procalcitonin levels swiftly fell to baseline.
One recent UK study examined the value of procalcitonin testing in broader patient ranges with positive results, though patient numbers were small [33]. Briefly, tests on 99 Medical Admissions Unit (i.e. emergency admission) patients with suspected infection led to antibiotics being denied - based on low procalcitonin levels - to 52. Although six of these individuals died during hospitalisation, none died of infection. A further 87 procalcitonin tests were performed on 42 intensive care cases, with antibiotics withheld on 42 occasions based on low procalcitonin levels. Five patients died of infection but none of these had been denied antibiotics. These data suggest wider scope to use procalcitonin to guide and rationalise antibiotic use. Nevertheless, procalcitonin is an imperfect biomarker, with levels also raised by trauma or surgery, complicating use in these patient groups [34]. Levels also are unhelpful e.g. in diagnosing appendicitis [35]. Some studies suggest that following procalcitonin trends is more useful than single snapshot measurements, precluding convenient use in community or emergency settings.
In the longer term, combinations of biomarkers may be more useful, and the technology to measure these is becoming available. For example Almansa et al [36] used gene chip technology to show increased transcription of a range of neutrophil proteases in patients with chronic obstructive pulmonary disease, finding that expression changes reflected the severity of disease. The same research group separately developed a severity score for sepsis patients based on the differential expression of various interleukins and cytokines [37].
Rapid identification of pathogens and their resistances
Whilst biomarker tests improve the recognition of patients with bacterial infection, they do nothing to accelerate identification of particular pathogens and resistances or to guide the choice of antibiotic. To do this, and to escape the time constraints of bacterial growth, it is necessary to apply nucleic acid or immunological technologies to the clinical specimen itself. This can be done, or has the potential to be done, at three levels, currently at various levels of development and deployment. Firstly, single or multiplex PCR can be used to seek specific pathogens, principally the agents of classical infectious diseases. Secondly, PCR can be used to seek ranges of likely pathogens in common clinical syndromes, along with critical resistances. Last, genomic sequencing can be used to provide a comprehensive analysis of the pathogens and their resistance genes.
Single PCR tests for specific pathogens are widely used. They include (i) nucleic acid amplification tests (NAATs) for gonococci and Chlamydia spp. in STI [38] (ii) and molecular diagnostics for tuberculosis [39, 40] (Table 1) (iii) and kits marketed (e.g. by Cepheid and BD) to aid infection control by identifying patients colonised e.g. by MRSA so that they can be isolated, cohorted and decolonised [41, 42]. Such kits, which generally use swab samples to detect colonisation, are now being evaluated for clinical fluids (i.e. blood, urine and respiratory secretions) for the characterisation of clinical infection [43, 44]. The obvious limitation is that they seek only single pathogens and resistances, and their main potential lies in screening or in outbreak investigation -answering the question e.g. 'Has this patient acquired the prevalent KPC Klebsiella?'
A further concern, specifically of the NAATs tests for STIs, is that they do not detect resistance in Neisseria gonorrhoeae [45]. Consequently, in settings where they replace rather than supplement culture-based bacteriology they may impede the surveillance of antibiotic resistance - an important public health concern in this species, which has a notorious reputation for evolution. Last, and depending on the particular fragment amplified, there may be a risk of false positives if the resistance gene is no longer functional; this has been an issue with some MRSA detection tests [46]; alternatively false negative results may arise if the target gene is altered so that it is no longer recognised, as happened with Chlamydia in Sweden [47].
Multiplex PCR systems (Table 2) seek the pathogens responsible for most cases of their target infection or syndrome, delivering results in 1-6 hours. Several, notably the Curetis Unyvero (http://www.curetis.com), Idaho FilmArray [48] and Luminex systems seek a few key resistances but aim, primarily, to answer the question 'What is the pathogen?', allowing early refinement of treatment. The amplification integral to PCR gives very sensitive detection, which is important in bacteraemia, where the bacterial count may be as few as 1-3 cfu/mL blood.
Experience is greatest with Roche's Septifast system, which can be seen as a useful prototype for the technology. Results have been mixed, with reported sensitivity and specificity between 50-90% [49-51] and with inconsistency on which species are best-detected. A complication is that blood culture, taken as the reference, is itself imperfect, with many studies finding that Septifast detected pathogens where culture failed. Thus, only 25/77 pathogens found by Lodes et al [52] using Septifast were also grown in blood culture although, strikingly, the same pathogens found by Septifast were grown from other body sites in a further 17 cases, suggesting that the multiplex was more sensitive than standard methodology. Lodes et al [52] also found that the rapid detection of pathogens by Septifast led to early adjustment of therapy in 16.9% of cases whilst, in an analysis for patients with septic shock, Alvarez et al [53] found a 20% reduction in total hospitalisation cost for patients whose therapy was guided by the method, though no reduction is total mortality. Further implementation studies are ongoing, including in the UK [54].
Whilst these data are encouraging, limitations are apparent. First and foremost, multiplex systems can only identify those pathogens and resistances for which they include relevant primers; other organisms and resistances are missed. This creates a limited problem for pathogen detection, since around 90% of bacteraemias or pneumoniae are caused by 10 pathogens or fewer but it does means that a negative result does not exclude infection. Non-comprehensiveness is a greater issue with respect of detecting resistance genes, since it is impossible to exclude all the genes that might engender resistance. What is more, PCR is not the ideal technology when resistance arises by mutation, particularly if multiple different changes can be involved, as with extended-spectrum TEM and SHV β-lactamases.
As a result of these caveats, multiplex PCRs are best equipped to detect patients with exceptionally resistant infections (e.g. by seeking a carbapenemase gene), needing non-standard antibiotics (e.g. colistin). They are less suitable for identifying those whose therapy can be de-escalated, given the difficulties of excluding the presence of all of the many resistance genes that might cause resistance. This means that they are more suited to optimise the treatment of individual patients than to support antibiotic stewardship. There also remains an economic barrier, in that a non-comprehensive test cannot replace existing methods of detection and antibiotic testing, meaning that molecular and classical methods must be run in parallel. Gains to the health system as a whole are overshadowed by immediate costs to the laboratory.
A further problem, for specimens from non-sterile sites, is the fact that DNA from multiple organisms may be mixed, making it hard to identify which organism is the pathogen and whether it hosts any resistance genes also found. If a resistance gene integrates at a particular point in the chromosome, as with mecA of MRSA, its host can be identified by PCR across the insertion site, as in Cepheid's GeneXpert system, but this strategy cannot resolve the hosts of plasmid-mediated genes.
These limitations are potentially overcome by next-generation sequencing [55], which is becoming increasingly available, as are the bioinformatic tools needed to analyse the massive amounts of data generated [2]. Sequence data can now be generated with benchtop instruments and, potentially, by much smaller devices, such as with the Oxford Nanopore technology [56]. Unlike PCR, sequencing has the potential to recognise all species and resistance genes within a matter of hours, and, by matching genomes, to track outbreak strains, as already illustrated for both MRSA [57] and Klebsiella pneumoniae with KPC carbapenemases [58].
The UK's Health Protection Agency is planning to use real time next-generation sequencing to analyse resistant bacteria referred from clinical practice and to sequence every one of the 10,000 to 20,000 Salmonella cultures referred annually from local laboratories - this may be extended to include animal strains to track the transmission through the food chain. A side-by-side comparison with traditional methods is scheduled to start in April 2013 and run for 3-12 months. This project, if successful, will go a long way to testing the potential of next generation sequencing and to establishing whether it is cheaper and better than existing culture-based methods, in particular for determining resistance profiles. Salmonella is a useful validation organism because of the level of knowledge of its genome but, if successful, there are real opportunities for the use of next-generation sequencing in much wider range of clinical infections.
Considerable challenges nevertheless remain before sequencing methodology can be deployed as a routine diagnostic. Some of these - cost and the availability of bioinformatic tools - are set to become diminishing issues with the rapid advance of the technology. Others are more fundamental. Most obviously - and this is an issue also for PCR - the correlation between resistance genotype and phenotype is imperfect. Detection of mecA reliably predicts of methicillin resistance in staphylococci and detection of blaTEM predicts ampicillin resistance in Escherichia coli. However the susceptibility of an E. coli with a β-lactamase gene to inhibitor combinations such as piperacillin-tazobactam varies not only on the type(s) of β-lactamase but also on how strongly these are expressed and on the expression of the porin genes [59]. Cefixime resistance in N. gonorrhoeae can reflect various combinations of multiple changes to penicillin-binding protein genes, porin genes and the promoter or coding sequences of the mtr efflux pump genes [60] (Table 3), whilst resistance to β-lactams in P. aeruginosa involves a variable geometry of up-regulated efflux pumps, partially-derepressed AmpC β-lactamase and porin loss [61]. Bioinformatic tools to predict resistance will need to take all these contributory factors into account and are unlikely to predict a precise MIC. This runs against the thinking of both the Clinical Laboratory Standards Institute and European Committee on Antimicrobial Susceptibility Testing, which have come to define susceptibility and resistance on increasingly precise pharmacodynamic criteria, rather than the presence of mechanisms [62].
In some cases, for example nitrofurantoin, daptomycin and polymyxin, also glycopeptide resistance in staphylococci, the exact genetic correlates of resistance remain unknown or debatable, precluding confident prediction from sequence data. Last, resistance occasionally involves new genes which will not reliably be identified from sequence data, though bioinformatic tools may predict their role if they have homology to known resistance genes.
Logistic barriers to molecular bacteriology
Rapid diagnostics will deliver greatest advantage if they are close to the patient, at the bedside or in the physician's office. This runs counter to the trend, widespread in the UK and Europe, also Australia of centralising bacteriology for multiple hospitals at single site, with specimens spending several hours in transport and distribution networks. One answer is to have a small local laboratory for molecular tests on urgent specimens whilst non-urgent specimens are transferred to a central laboratory and processed by high throughput classical bacteriology. This might be cost-effective and would support treatment of individual patients, but the potential of molecular methods to improve stewardship would be lost if only a few patients have these tests done.
Last, for non-comprehensive PCR-based methods and at least initially for sequencing, it will be necessary to run classical methodology in parallel, adding cost to the laboratory budget, whilst any savings and advantage accrue elsewhere in the healthcare system. Over time only the collective experience of using the new genomic approaches alongside extant methodology will determine their impact.
Conclusions
This short review has sought to outline the potential gains and challenges to accelerating clinical bacteriology by use of biomarker tests and rapid molecular diagnostics for pathogen characterisation.
Whilst the barriers to deployment are considerable they should not disguise the major gains to be had and the fact that advances in molecular biology, particularly next-generation sequencing, are making these increasingly accessible. Not only will individual patients and stewardship benefit from early tailoring of treatments but, in addition, there will be scope to run trials of novel narrow-spectrum antibiotics, with carefully-selected patients enrolled before they have received other antibiotics, making them ineligible for inclusion. Looking forwards, it is possible that molecular diagnostics will change the shape of the antibiotic market, driving the use of narrow spectrum agents likely to cause less harmful disruption of the gut flora.
Last, it should be appreciated that current culture-based bacteriology is a poorer gold standard than often supposed. Not only is it slow but, additionally, it commonly fails to grow pathogens from patients with clinical evidence of infection. Pathogens are cultured successfully from only 30-40% of haematology patients with suspected bacteraemia [63] and, in pneumonia trials, the number of clinically-diagnosed patients is often double or triple those from whom a pathogen is successfully cultured and characterised [64]. In routine practice, such patients continue to be treated blind, often excessively but sometimes inadequately. Molecular methods do not need to be perfect to offer an improvement over this status quo.
Transparency Declaration
DML has shareholdings in Dechra, Eco Animal Health, Merck and Pfizer and has accepted grants, speaking invitations and conference invitations from Pfizer, Novartis, AstraZeneca and Astellas and has advisory or consultancy relationships with Achaogen, Adenium, Allecra, AstraZeneca, Basilea, Bayer, Cubist, Curetis, Discuva, GlaxoSmithKline, Kalidex, McKinsey, Meiji, Pfizer, Roche, Tetraphase, Theravance and Wockhardt. JW is a non-executive director of Discuva Ltd.



 XML Download
XML Download