

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Acinetobacter baumannii infections have become significant pathogen in hospitalized patients, especially in the intensive care unit setting. Community-acquired Acinetobacter meningitis in adults is a very rare infection of the central nervous system. Most community-acquired Acinetobacter infections have been reported from countries with a tropical or subtropical climate. Acinetobacter infections mainly affect patients with some form of comorbidity and are also associated with heavy smoking and excess alcohol consumption. In our case, a 62-year-old male patient with DM, hypertension, and excess alcohol consumption developed meningitis. Bulging membrane and inflammation were observed in the right ear. A. baumannii meningitis was confirmed by blood, CSF, and ear discharge culture. The patient was treated effectively with meropenem for 21 days. After antibiotic treatment, follow-up cultures of CSF, blood, and ear discharge showed a negative result, and the CSF cell profile was normalized. However, the patient died of recurrent pneumonia on hospital day 45. We report on a case of community-acquired Acinetobacter meningitis in an adult in Korea.
Figures and Tables
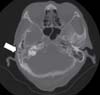 | Figure 1Brain CT shows acute otitis media and mastoiditis, right (arrow). Opacified air cells and fluid are identified in the middle ear and mastoid.
|
 | Figure 2Gram stain on CSF shows gram negative bacilli (arrow). (H&E stain, ×1,000 Cerebrospinal fluid).
|
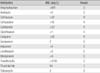
Table 1
Based on Culture Tests for Blood, CSF, and Otorrhea, A. baumannii was Identified. Results of the Sensitivity Test
![]()
Table 2
Review of Reported Cases of Community-acquired Acinetobacter Infection in South Korea

N/D, no data
aOne case of Asian Network for Surveillance of Resistant Pathogens (ANSORP) Study Group community-acquired pneumonia caused by gram-negative bacilli.
bThe patient was diagnosed as having multiple rib fractures and hemothorax, and was found dead in his house three days later. At autopsy, the pneumothorax test showed a positive result, due to pleural adhesion and cavitary abscess from A. baumannii pneumonia.
![]()
References
1. Seifert H, Baginski R, Schulze A, Pulverer G. The distribution of Acinetobacter species in clinical materials. Zentralbl Bakteriol. 1993. 279:544–552.
2. Morris A, Low DE. Nosocomial bacterial meningitis, including central nervous shunt infections. Infect Dis Clin North Am. 1999. 13:735–750.

3. Anstey NM, Currie BJ, Hassell M, Palmer D, Dwyer B, Seifert H. Community-acquired bacteremic Acinetobacter pneumonia in tropical Australia is caused by diverse strains of Acinetobacter baumannii, with carriage in the throat in at-risk groups. J Clin Microbiol. 2002. 40:685–686.
4. Durand ML, Calderwood SB, Weber DJ, Miller SI, Southwick FS, Caviness VS, Swartz MN. Acute bacterial meningitis in adults: a review of 493 episodes. N Engl J Med. 1993. 328:21–28.
5. Sigurdardóttir B, Björnsson OM, Jónsdóttir KE, Erlendsdóttir H, Gudmundsson S. Acute bacterial meningitis in adults. A 20-year overview. Arch Intern Med. 1997. 157:425–430.
6. Lu CH, Chang WN, Chung YC, Chang HW. The prognostic factors of gram-negative bacillary meningitis. J Hosp Infect. 1998. 40:27–34.
7. Bergogne-Bérézin E, Towner KJ. Acinetobacter spp. as nosocomial pathogens: microbiological, clinical, and epidemiological features. Clin Microbiol Rev. 1996. 9:148–165.
8. Falagas ME, Karveli EA, Kelesidis I, Kelesidis T. Community-acquired Acinetobacter infections. Eur J Clin Microbiol Infect Dis. 2007. 26:857–868.
9. Lu CH, Huang CR, Chang WN, Chang CJ, Cheng BC, Lee PY, Lin MW, Chang HW. Community-acquired bacterial meningitis in adults: the epidemiology, timing of appropriate antimicrobial therapy, and prognostic factors. Clin Neurol Neurosurg. 2002. 104:352–358.
10. Leung WS, Chu CM, Tsang KY, Lo FH, Lo KF, Ho PL. Fulminant community-acquired Acinetobacter baumannii pneumonia as a distinct clinical syndrome. Chest. 2006. 129:102–109.
11. Han SH, Na DJ, Yoo YW, Kim DG, Moon YR, Moon KM, Lee YD, Cho YS, Han MS, Yoon HJ. A case of probable community acquired Acinetobacter baumannii pneumonia. Tuberc Respir Dis. 2007. 63:273–277.
12. Kang CI, Song JH, Oh WS, Ko KS, Chung DR, Peck KR. Asian Network for Surveillance of Resistant Pathogens (ANSORP) Study Group. Clinical outcomes and risk factors of community-acquired pneumonia caused by gram-negative bacilli. Eur J Clin Microbiol Infect Dis. 2008. 27:657–661.
13. Na JY, Min BW, Chung SH, Kim MY, Lee YJ, Park JT, Kim HS. A probable community-acquired pneumonia due to Acinetobacter baumannii infection presenting the positive pneumothorax test at autopsy. Korean J Leg Med. 2010. 34:125–128.
14. Lee Y, Yoon S, Lee HS, Kang BH, An J, Kim YJ, Hong SB, Choi SH. A case of severe community-acquired Acinetobacter baumannii pneumonia with bacteremia. Infect Chemother. 2012. 44:71–74.
15. Chang WN, Lu CH, Huang CR, Chuang YC. Community-acquired Acinetobacter meningitis in adults. Infection. 2000. 28:395–397.
16. Lowman W, Kalk T, Menezes CN, John MA, Grobusch MP. A case of community-acquired Acinetobacter baumannii meningitis has the threat moved beyond the hospital? J Med Microbiol. 2008. 57:676–678.
17. Ozaki T, Nishimura N, Arakawa Y, Suzuki M, Narita A, Yamamoto Y, Koyama N, Nakane K, Yasuda N, Funahashi K. Community-acquired Acinetobacter baumannii meningitis in a previously healthy 14-month-old boy. J Infect Chemother. 2009. 15:322–324.
 XML Download
XML Download