

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Nasopharyngeal bacterial flora can cause respiratory tract diseases as well as invasive bacterial diseases. Moraxella catarrhalis colonizing in the nasopharynx is considered an important potential pathogen with an increasing production of β-lactamase. This study examined the nasopharyngeal colonization rate of M. catarrhalis and the antibiotic susceptibility of M. catarrhalis.
Materials and Methods
Healthy children who visited one of the three University hospitals in the Republic of Korea or attended a day-care center around the participating hospitals were enrolled in this study. The nasopharyngeal samples were obtained by nasopharyngeal washing with normal saline and M. catarrhalis was isolated. The nasopharyngeal colonization rate of M. catarrhalis was investigated and the minimal inhibitory concentrations (MICs) were measured for commonly used oral antibiotics (amoxicillin, amoxicillin/clavulanate, cefaclor, cefixime, cefdinir, cefditoren, erythromycin and trimethoprim).
Results
Three hundred and seventy-nine children aged between 6 months and 5 years were enrolled, and the nasopharyngeal colonization rate of M. catarrhalis was 33% (124 children). All isolated M. catarrhalis produced β-lactamase. The MIC90 of the antibiotics were as follows: amoxicillin, >16 mg/L; amoxicillin/clavulanate, 0.5 mg/L; cefaclor, 8 mg/L ; cefixime, 0.125 mg/L; cefdinir, 0.25 mg/L; cefditoren, 0.25 mg/L; erythromycin, 0.5 mg/L; and trimethoprim, >16 mg/L.
Figures and Tables
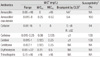
Table 1
Proportions of Children with Nasopharyngeal Colonization of Moraxella catarrhalis and Those without Colonization

![]()
References
1. García-Rodríguez JA, Fresnadillo Martínez MJ. Dynamics of nasopharyngeal colonization by potential respiratory pathogens. J Antimicrob Chemother. 2002. 50:Suppl S2. 59–73.

2. Berner R, Schumacher RF, Brandis M, Forster J. Colonization and infection with Moraxella catarrhalis in childhood. Eur J Clin Microbiol Infect Dis. 1996. 15:506–509.
3. De Lencastre H, Kristinsson KG, Brito-Avô A, Sanches IS, Sá-Leão R, Saldanha J, Sigvaldadottir E, Karlsson S, Oliveira D, Mato R, Aires de Sousa M, Tomasz A. Carriage of respiratory tract pathogens and molecular epidemiology of Streptococcus pneumoniae colonization in healthy children attending day care centers in Lisbon, Portugal. Microb Drug Resist. 1999. 5:19–29.
4. Quiñones D, Llanes R, Toraño G, Pérez M. Nasopharyngeal colonization by Moraxella catarrhalis and study of antimicrobial susceptibility in healthy children from Cuban day-care centers. Arch Med Res. 2005. 36:80–82.
5. Mackenzie GA, Leach AJ, Carapetis JR, Fisher J, Morris PS. Epidemiology of nasopharyngeal carriage of respiratory bacterial pathogens in children and adults: cross-sectional surveys in a population with high rates of pneumococcal disease. BMC Infect Dis. 2010. 10:304.
6. American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004. 113:1451–1465.
7. Vergison A. Microbiology of otitis media: a moving target. Vaccine. 2008. 26:Suppl 7. G5–10.
8. Casey JR, Pichichero ME. Changes in frequency and pathogens causing acute otitis media in 1995-2003. Pediatr Infect Dis J. 2004. 23:824–828.
9. Casey JR, Adlowitz DG, Pichichero ME. New patterns in the otopathogens causing acute otitis media six to eight years after introduction of pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2010. 29:304–309.
10. Faden H, Duffy L, Wasielewski R, Wolf J, Krystofik D, Tung Y. Relationship between nasopharyngeal colonization and the development of otitis media in children. Tonawanda/Williamsville Pediatrics. J Infect Dis. 1997. 175:1440–1445.
11. Revai K, Mamidi D, Chonmaitree T. Association of nasopharyngeal bacterial colonization during upper respiratory tract infection and the development of acute otitis media. Clin Infect Dis. 2008. 46:e34–e37.
12. Syrjänen RK, Auranen KJ, Leino TM, Kilpi TM, Mäkelä PH. Pneumococcal acute otitis media in relation to pneumococcal nasopharyngeal carriage. Pediatr Infect Dis J. 2005. 24:801–806.
13. Kim SM, Hur JK, Lee KY, Shin YK, Park SE, Ma SH, Min AY, Kang JH. Epidemiological study of pneumococcal nasal carriage and serotypes among Korean children. Korean J Pediatr. 2004. 47:611–616.
14. Kim KH, Hong JY, Lee H, Kwak GY, Nam CH, Lee SY, Oh E, Yu J, Nahm MH, Kang JH. Nasopharyngeal pneumococcal carriage of children attending day care centers in Korea: comparison between children immunized with 7-valent pneumococcal conjugate vaccine and non-immunized. J Korean Med Sci. 2011. 26:184–190.
15. Clinical and Laboratory Standards Institute. Document M100-S20. Haemophilus influenzae and Haemophilus parainfluenzae. Performance standards for antimicrobial susceptibility testing; 20th informational supplement. 2010. 30. Wayne, PA: CLSI;80–83.
16. Murphy TF, Parameswaran GI. Moraxella catarrhalis, a human respiratory tract pathogen. Clin Infect Dis. 2009. 49:124–131.
17. McGregor K, Chang BJ, Mee BJ, Riley TV. Moraxella catarrhalis: clinical significance, antimicrobial susceptibility and BRO beta-lactamases. Eur J Clin Microbiol Infect Dis. 1998. 17:219–234.
18. Broides A, Dagan R, Greenberg D, Givon-Lavi N, Leibovitz E. Acute otitis media caused by Moraxella catarrhalis: epidemiologic and clinical characteristics. Clin Infect Dis. 2009. 49:1641–1647.
19. Verduin CM, Hol C, Fleer A, van Dijk H, van Belkum A. Moraxella catarrhalis: from emerging to established pathogen. Clin Microbiol Rev. 2002. 15:125–144.
20. Berk SL, Kalbfleisch JH. The Alexander Project Collaborative Group. Antibiotic susceptibility patterns of community-acquired respiratory isolates of Moraxella catarrhalis in western Europe and in the USA. J Antimicrob Chemother. 1996. 38:Suppl A. 85–96.
21. Hsu SF, Lin YT, Chen TL, Siu LK, Hsueh PR, Huang ST, Fung CP. Antimicrobial resistance of Moraxella catarrhalis isolates in Taiwan. J Microbiol Immunol Infect. 2012. 45:134–140.
22. Gunnarsson RK, Holm SE, Söderström M. The prevalence of potential pathogenic bacteria in nasopharyngeal samples from healthy children and adults. Scand J Prim Health Care. 1998. 16:13–17.
23. van Gils EJ, Veenhoven RH, Rodenburg GD, Hak E, Sanders EA. Effect of 7-valent pneumococcal conjugate vaccine on nasopharyngeal carriage with Haemophilus influenzae and Moraxella catarrhalis in a randomized controlled trial. Vaccine. 2011. 29:7595–7598.
24. Jourdain S, Smeesters PR, Denis O, Dramaix M, Sputael V, Malaviolle X, Van Melderen L, Vergison A. Differences in nasopharyngeal bacterial carriage in preschool children from different socio-economic origins. Clin Microbiol Infect. 2011. 17:907–914.
25. Pingault NM, Bowman JM, Lehmann D, Riley TV. Antimicrobial susceptibility of Moraxella catarrhalis isolated from children in Kalgoorlie-Boulder, Western Australia. Pathology. 2010. 42:273–279.
26. Harrison CJ, Woods C, Stout G, Martin B, Selvarangan R. Susceptibilities of Haemophilus influenzae, Streptococcus pneumoniae, including serotype 19A, and Moraxella catarrhalis paediatric isolates from 2005 to 2007 to commonly used antibiotics. J Antimicrob Chemother. 2009. 63:511–519.
27. Ahmad F, McLeod DT, Croughan MJ, Calder MA. Antimicrobial susceptibility of Branhamella catarrhalis isolates from bronchopulmonary infections. Antimicrob Agents Chemother. 1984. 26:424–425.
 XML Download
XML Download