

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Recently, the incidence of candida infection has increased. Candida species often show hematogenous spread to the kidney, brain, heart, and eyes. And delayed onset of hematogenous spread is relatively rare. A 53-year-old female patient was admitted with left anterior chest pain with swelling and mild fever. She had been treated successfully with fluconazole for candidemia caused by C. albicans eight month ago. On admission chest CT scan revealed multiple subcutaneous abscesses involving the anterior chest. Percutaneous drainage of the abscess was performed. C. albicans was isolated from drained pus. Treatment with fluconazole did not to improve the abscess; therefore, micafungin and voriconazole were administered as a replacement. The patient recovered after 10-week administration.
Figures and Tables
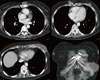
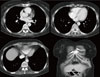
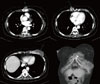 | Figure 1Initial contrast-enhanced CT scan shows multiple subcutaneous abscesses involving the anterior chest (An abscess measuring 8.0×6.4×5.4 cm just below the left breast, an abscess measuring 3.0×1.7 cm adjacent to the right xiphoid process, and an abscess measuring 3.6×2.5 cm attached to the sternum).
|
References
1. Kwon SJ, Park WC, Rhee JK, Yun KJ. Systemic infection by the gastric candidiasis. J Korean Surg Soc. 2003. 64:510–514.
2. Cohen R, Roth FJ, Delgado E, Aheam DG, Kasler MH. Fungal flora of the normal human small and large intestine. N Eng J Med. 1969. 280:638–641.

3. Oh BJ, Choi HW, Lee JS, Cho D, Kee SJ, Shin MG, Shin JH, Suh SP, Ryang DW. Clinical and laboratory features of candidemia caused by different Candida species. Korean J Lab Med. 2005. 25:317–323.
4. Kao AS, Brandt ME, Pruitt WR, Conn LA, Perkins BA, Stephens DS, Baughman WS, Reingold AL, Rothrock GA, Pfaller MA, Pinner RW, Hajjeh RA. The epidemiology of candidemia in two United States cities: results of a population-based active surveillance. Clin Infect Dis. 1999. 29:1164–1170.
5. Wey SB, Mori M, Pfaller MA, Woolson RF, Wenzel RP. Hospital acquired candidemia. The attributable mortality and excess length of stay. Arch Intern Med. 1988. 148:2642–2645.
6. Verduyn Lunel FM, Meis JF, Voss A. Nosocomial fungal infections: candidemia. Diagn Microbiol Infect Dis. 1999. 34:213–220.
7. Lee MK, Park BG. Rapid identification of Candida albicans by 'Spiking' on blood and chocolate agar plates. Korean J Clin Microbiol. 2007. 10:150–153.
8. Dignani MC, Solomkin JS, Anaissie EJ. Anaissie EJ, McGinnis MR, Pfaller MA, editors. Candida. Clinical Mycology. 2003. Philadelphia: Churchill Livingstone;195–239.
9. Edwards JE. Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J, editors. Candidiasis. Harrison's Principles Of Internal Medicine. 2008. 17th ed. New York: McGraw Hills;1254–1256.
10. Lee SM, Kim MK, Lee JL, Wee WR, Lee JH. Experience of comamonas acidovorans keratitis with delayed onset and treatment response in immunocompromised cornea. Korean J Ophthalmol. 2008. 22:49–52.
11. Lee KH, Kim MR. A clinical study on nosocomial candidemia. Korean J Infect Dis. 1998. 30:45–53.
12. Kim M, Lee J, Chung CS, Jang JH, Ahn BM, Song W. A case of psoas abscess caused by Candida glabrata. Infect Chemother. 2010. 42:43–47.
13. Fukuhara S, Nishimura K, Yoshimura K, Okuyama A, Yamato M, Kawamori D, Matsuhisa M. A case of psoas abscess caused by Candida albicans. Hinyokika Kiyo. 2003. 49:141–143.
14. Noh JY, Heo JY, Choi WS, Jo YM, Song JY, Cheong HJ, Kim WJ. Candida spondylodiscitis with epidural abscess treated with voriconazole. Korean J Med Mycol. 2009. 14:145–149.
15. Pfaller MA, Diekema DJ, Gibbs DL, Newell VA, Meis JF, Gould IM, Fu W, Colombo AL, Rodriguez-Noriega E. Global Antifungal Surveillance Study. Results from the ARTEMIS DISK Global Antifungal Surveillance study, 1997 to 2005: an 8.5-year analysis of susceptibilities of Candida species and other yeast species to fluconazole and voriconazole determined by CLSI standardized disk diffusion testing. J Clin Microbiol. 2007. 45:1735–1745.
16. Lee JS, shin JH, Lee K, Kim MN, Shin BM, Wh Y, Lee WG, Lee HS, Chang CL, Kim SH, Shin MG, Suh SP, Ryang DW. Specieds distribution and susceptibility to azole antifungals of Candida bloodstream isolates form eight university hospitals in Korea. Yonsei Med J. 2007. 48:779–786.
17. Tumbarello M, Sanguinetti M, Trecarichi EM, La Sorda M, Rossi M, de Carolis E, de Gaetano Donati K, Fadda G, Cauda R, Posteraro B. Fugaemia caused by Candida glabrata with reduced susceptibility to fluconazole due to altered gene expression: risk factors, antifungal treatment and outcome. J Antimicrob Chemother. 2008. 62:1379–1385.
18. Maenza JR, Merz WG, Romagnoli MJ, Keruly JC, Moore RD, Gallant JE. Infection due to fluconazole-resistant Candida in patients with AIDS: prevalence and microbiology. Clin Infect Dis. 1997. 24:28–34.
19. Cruciani M, Serpelloni G. Management of Candida infections in the adult intensive care unit. Expert Opin Pharmacother. 2008. 9:175–191.
20. Levêque D, Nivoix Y, Jehl F, Herbrecht R. Clinical pharmacokinetics of voriconazole. Int J Antimicrob Agents. 2006. 27:274–284.
 XML Download
XML Download