

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Occurrence of severe sepsis, which accounts for 10-30% of intensive care unit (ICU) admissions worldwide, is relatively common [1-4]. While severe sepsis is a deadly medical condition, previous studies involving large observational cohorts have reported an overall rate of mortality ranging between 28.6-56.0% [5, 6]. Many factors can be determinants of poor outcome in patients with severe sepsis; we argue that there are too many to apply in real clinical situations. Typically, the list includes age, severity of a patient's underlying disease, number of dysfunctional organ systems, severity of the illness, hypothermia, thrombocytopenia, lactic acidosis, multiple sources of infection, positive blood cultures, and type of organism [6, 7].
In most studies of severe sepsis, patients were not stratified according to whether the infection was community-acquired vs. hospital acquired or bacteremic vs. non-bacteremic. Previous studies of bacteremic diseases have focused on individual organisms or combined community- and hospital-acquired bacteremia [8, 9]. One study suggested an association of patient outcomes in cases of severe community-acquired bacteremic sepsis with scores for albumin and Acute Physiology and Chronic Health Evaluation II (APACHE II) [10]; however, more data are needed in order to validate these earlier findings.
Epidemiological and prognostic factors associated with severe community-acquired bacteremic sepsis could differ from those of hospital-acquired and/or non-bacteremic cases, and could inform treatment recommendations and aid in establishment of national health policies. Our aim in this study was to describe the clinical and microbiological characteristics of patients with severe community-acquired bacteremic sepsis, and to determine which of these variables are associated with mortality.
Materials and Methods
1. Study design and patients
A prospective, multicenter, observational study was conducted in the medical (n=12) and surgical (n=10) intensive care units (ICUs) of 12 university-affiliated teaching hospitals in the Republic of Korea from April, 2005 to February, 2009. A prospective analysis was conducted using data from adult patients (18 years and older) with severe community-acquired bacteremic sepsis who had been recently admitted to the ICUs of the participating centers. Patient follow-up continued until death or discharge from the hospital. Cases involving recurrence or relapse were excluded. There was no standardized intervention associated with management of sepsis, and physicians followed routine medical practices in treatment of their patients.
Prior to initiation of the study, the protocol was reviewed and approved by the institutional review board from each participating center.
2. Definitions
In this study, for diagnosis of severe sepsis, we used criteria developed by Bernard et al. [11, 12], as well as hepatic dysfunction (serum bilirubin >21 µmol/L), gastrointestinal dysfunction (stress upper gastrointestinal bleeding), and mental change (Glasgow coma scale ≤13). Diagnosis of severe sepsis required evidence of infection and at least two systemic inflammatory response syndrome conditions and at least one organ system dysfunction. Septic shock was diagnosed as sepsis with sustained hypotension lasting at least one hour despite adequate fluid resuscitation or as sepsis requiring vasopressors for maintenance of adequate systolic blood pressure [11]. Severe community-acquired sepsis was defined as the presence of severe sepsis upon admission or sepsis that developed within 24 hours of admission. According to the previously mentioned criteria, cases involving nosocomial infection were excluded [13]. Infections that became evident <48 hours after discharge from the hospital were deemed nosocomial [13]. Determination of the primary site of infection was based on the organs affected and was classified as one of the following: lower respiratory tract, intra-abdominal, genitourinary tract, skin and soft tissue, central nervous system, or primary bloodstream infection, which was defined as a positive blood culture without focus.
Isolation of one or more viable microorganisms from blood cultures resulted in diagnosis of bacteremia. Isolation of common skin-dwelling organisms, such as coagulase-negative Staphylococcus species and Bacillus species, from two or more blood cultures from a suspected patient was considered significant. The final diagnosis was made by infectious disease specialists.
Initial empirical antibiotic therapy was defined as appropriate when antibiotics were started intravenously with optimal dosing and intervals within 24 hours after recognition of severe sepsis or septic shock, and the infecting microorganism was subsequently found to be susceptible in vitro to the antibiotics administered.
3. Data collection
For the first 24 hours following admission, data for each patient were collected using the standardized web-based case report form via the website of the Korean Society of Infectious Diseases. Data included demographic characteristics, co-morbid medical conditions, as determined by Charlson's comorbidity index [14], factors predisposing to infection, primary site of infection, APACHE II scores [15], and diagnosis of severe sepsis, septic shock, and organ dysfunction. Sepsis-related Organ Failure Assessment (SOFA) scores [16], microorganism isolates, and hospital mortality data were also collected at admission.
4. Statistical analyses
The Chi-square test or Fisher's exact test was used for comparison of categorical variables. Continuous variables were expressed as means±standard deviations, and t-tests were performed for comparison of means. For determination of independent factors sociated with mortality, variables that showed a significant association with in-hospital mortality in univariate analysis were further analyzed using multivariate logistic regression analysis. Statistical significance was defined as a two-tailed P value<0.05.
SPSS version 13.0 (SPSS Inc., Chicago, IL, USA) was used in performance of statistical analyses.
Results
1. Patient characteristics
During the study period, data from 1,357 cases were collected and 1,152 patients were diagnosed with severe community-acquired sepsis. Among them, 422 patients documented as having severe community-acquired bacteremic sepsis were subsequently included in this study (Fig. 1). While occurrence of all-cause in-hospital mortality was observed in 121 patients (28.7%), 7-day and 28-day mortality rates were 14.9% (63 of 422) and 24.6% (104 of 422), respectively. The mean hospital stay was 3.96±93.08 days (range 0-939, median 16 days).
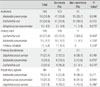
Sex distribution was nearly equal, and the mean age (years) of patients was 64.6±14.3 (range 18-97, median 66). Underlying disease was observed in 300 patients (71.1%), with a mean Charlson score index of 1.6±1.3 (range 0-9). Detailed comorbidity and severity parameters for the enrolled patients are shown in Table 1. Initially detected major clinical manifestations were as follows: hypotension (58.3%), hematologic dysfunction (58.3%), renal dysfunction (41.2%), liver dysfunction (37.4%), mental change (36.0%), respiratory failure (32.5%), metabolic acidosis (29.6%), cardiac dysfunction (13.5%), and gastrointestinal bleeding (3.3%). The mean number of organ dysfunctions was 2.7±1.6 (range, 0-7).
2. Primary site of infection
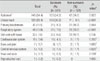
The most common primary site of infection was intra-abdominal (34.4%), followed by the urinary tract (28.4%), primary bloodstream (11.1%), and respiratory tract (10.9%). In-hospital mortality due to respiratory tract, primary bloodstream, skin and soft tissue, intra-abdominal, cardiovascular, and urinary tract infections was 54.3%, 46.8%, 39.4%, 29.0%, 13.3%, and 9.2%, respectively (Table 2).
3. Microbiology
Compared with Gram-positive bacteria (25.1%), a greater percentage of pathogens were Gram-negative bacteria (72.0%). Polymicrobial infections and anaerobic infections accounted for 2.8% and 0.2% of infections, respectively. Among Gram-negative microorganisms, the most common pathogen was Escherichia coli (37.7%), followed by Klebsiella pneumoniae (22.0%). The most common Gram-positive pathogen was Staphylococcus aureus (11.8%), followed by Streptococcus pneumoniae (10.2%). The top three common causative microorganisms according to primary site of infection are shown in Table 3.
4. Independent risk factors for in-hospital mortality
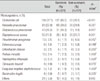
In univariate analysis of the demographic and clinical characteristics of patients and their severity of illness, the APACHE II score and the number of organ dysfunctions differed significantly between survivors and non-survivors (Table 1). Only a small proportion of patients (32/422, 7.6%) received inappropriate antibiotic treatment; therefore, inadequate initial antimicrobial treatment might not contribute to in-hospital mortality. Mortality rate is higher for patients with sepsis associated with respiratory tract infection, primary bloodstream infection, or caused by Pseudomonas aeruginosa or S. aureus, while a lower mortality rate was observed for patients with urinary tract infections and E. coli as a pathogen (Tables 2 and 4).
Multivariate logistic regression analysis was performed for further analysis of significant parameters found by univariate analyses. Respiratory tract infection (odds ratio [OR], 2.60; 95% confidence interval [CI], 1.11-6.09), number of organ system dysfunctions (OR, 1.39; 95% CI, 1.13-1.71), and APACHE II score (OR, 1.08; 95% CI, 1.03-1.13) showed an association with a greater risk of death, whereas E. coli bacteremia (OR, 0.31; 95% CI, 0.16-0.64) was associated with a lower risk. Independent risk factors associated with 7-day and 28-day mortality in multivariate logistic regression analysis are shown in Table 5.
Discussion
In the present study, all-cause in-hospital mortality was 28.7% (121 of 422 patients). Patients who presented with shock showed a slightly lower rate of mortality (26.9%) than patients without shock. As reported in previous studies, mortality resulting from severe sepsis ranged from 28.6-56.0%, and mortality rate for patients with septic shock were higher (40-70%) than those of patients with sepsis alone (25-30%) [3, 5, 6, 17, 18]. In a study of patients with severe community-acquired bacteremic sepsis, Artero et al. reported an all-cause in-hospital mortality rate of 34.4% [10], higher than the mortality rate recorded in this study. The modest result for general mortality and the unexpected result for lower mortality in patients with shock may be due to inclusion of cases with different disease severities, as reflected by APACHE II scores, compared to the previous study (19.4 in our study vs. 22.0 in the other study), as well as a disparity in the most common site of primary infection (urinary tract infection in our study vs. respiratory tract infection in the previous study) [10].
Our finding that E. coli was the most common isolate from patients with severe community-acquired bacteremic sepsis (159 of 422, 37.7%) is in agreement with results reported by Diekema et al. [19]. However, other studies have reported a general, worldwide increase in occurrence of Gram-positive infections, such as S. aureus infections [10, 20, 21]. Differences in proportions of causative organisms may be the result of differences in the primary focus of infection. Mylotte et al. [20] reported pneumonia as the most common site of infection. However, in our study, the most common primary site of infection was intra-abdominal (34.4%), followed by the urinary tract (28.4%), primary bloodstream (11.1%), and respiratory tract (10.9%). Consistent with the findings of other studies, we found that lower respiratory tract infection, severity of illness upon admission, and the presence of multiple organ dysfunctions were the major factors associated with a poor prognosis in Korean patients with severe community-acquired bacteremic sepsis [8, 10, 20, 22, 23]. Infection with E. coli showed an association with lower mortality, which is also consistent with results reported by another study [24]. No significant association was observed between inadequate empirical antimicrobial treatment and higher mortality. However, administration of inadequate empirical antimicrobial treatment to critically ill patients with bloodstream infections has been reported as a key prognostic factor leading to a poor outcome [25, 26]. Discordance between results of our study and those of previous studies might be attributed to the fact that, in our study, only a few patients (7.6%) received inappropriate initial antibiotic treatment. The low rate of inadequate antimicrobial treatment may be due to the nature of the involved hospitals; all patients were recruited from university-affiliated teaching hospitals with specialists in infectious disease on staff.
This study had several limitations. First, it was performed within the ICUs of 12 university-affiliated teaching hospitals having a low prevalence of inadequate antimicrobial treatment. Therefore, it may be that the results of this study cannot be generalized to other hospitals. Second, it was an observational study, and, even though there was no standardized intervention for management of sepsis at different hospitals, the study center was not included as a separate variable. Nevertheless, specialists in infectious disease, especially those trained to care for critically ill patients, participated in management of these patients. Third, our patient cohort did not include a consecutive series of ICU patients with community-acquired infections, which may have led to selection bias for more severe infections, with a higher likelihood of mortality. However, there is no reason to believe that this would have changed the predisposing factors associated with mortality.
In conclusion, we found that disease severity, based on both the number of organ system dysfunctions and APACHE II score, in addition to microbiological factors and primary site of bacteremia, are in-hospital prognostic determinants of outcome in patients with severe community-acquired bacteremic sepsis in Korea.



 XML Download
XML Download