

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Infectious spondylitis (IS) is a rare infectious disorder, which is often associated with significant neurologic deficits and mortality. However, previous domestic studies, have paid more attention to the differential diagnosis between pyogenic spondylitis (PS) and tuberculous spondylitis (TS) rather than to the treatment and outcomes of them. The aims of this study were to determine the clinical manifestations and outcomes of IS and to determine its prognostic factors.
Materials and Methods
We compared the predisposing factors or associated illnesses and the clinical, radiological and laboratory features of the microbiologically confirmed cases of PS and TS in a tertiary hospital from January 2004 to December 2009. We also analyzed the treatment outcomes and prognostic factors.
Results
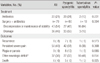
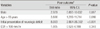
Of the 116 patients (78 males and 38 females), 93 (39 definite and 54 possible cases) had PS and 23 patients had TS. The patients with PS had a significantly higher rate of fever and higher levels of a WBC, CRP and ESR at the initial presentation than did the TS patients (P<0.05). TS was frequently associated with active tuberculosis of other organs and involvement of thoracic vertebral lesions. Among the 116 cases, 104 cases (83 PS cases, 21 TS cases) had followed-up. The mean duration of intravenous antibiotics treatment was 6.3 weeks (range: 0.8-16.0) for the PS patients, and the mean duration of anti-tuberculosis treatment was 36.0 weeks (range: 1.3-81.4 weeks) in the TS patients The proportion of favorable outcomes (complete recovery) was 34% and the proportion of poor ones was 66% (partial recovery with sequelae [60%] and death [6%]). The poor outcome of IS were independently associated with an age >65 years (OR=3.88, 95% CI=1.28-11.71, P=0.016) and an initial presentation of neurologic deficits (OR=8.69, 95% CI= 2.86-26.39, P<0.001).
Conclusions
The prognosis of the patients with IS was poor with partial recovery and sequelae in 60% of the patients and the mortality was 6%. The optimal treatment consisting of antibiotics and surgical treatment was needed to prevent poor outcomes of IS, and especially for the patients with an age >65 years and who displayed neurologic deficits at the initial presentation.
Figures and Tables
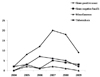 | Figure 1Yearly distribution of pyogenic spondylitis and tuberculous spondylitis according to the causative organisms from 2004 to 2009.
|
Table 1
Microbiological Distribution of the Causative Organisms for Infectious Spondylitis

MSSA, methicillin-susceptible Staphylococcus aureus; MRSA, methicillin-resistent Staphylococcus aureus.
aEscherichia coli (12 cases), Klebsiella pneumoniae (3 cases), Pseudomonas aeruginosa (2 cases), and Serratia marcescens (1 case).
bBrucella species (3 cases), Bacteroides fragilis (1 case), Neisseria species (1 case), and Candida parapsilosis (1 case).
![]()

Table 3
The Initial Manifestations, Laboratory findings and Radiologic findings according to the Type of Spondylitis

![]()
Table 4
Comparison of Treatment and the Clinical Outcomes: Pyogenic Spondylitis Versus Tuberculous Spondylitis
![]()
Table 5
Prognostic Factors on the Univariate Analysis of the Clinical Outcomes for the Patients with Infectious Spondylitis

WBC, white blood cell; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
aIntractable pain, persistent neurologic deficits (radiculopathy, paresis, plegia and loss of voiding and the sense of defecation) and death despite appropriate treatment were defined as a poor outcome.
bSurgical treatment for spinal biopsy (n=3) was excluded.
![]()
References
1. Grammatico L, Baron S, Rusch E, Lepage B, Surer N, Desenclos JC, Besnier JM. Epidemiology of vertebral osteomyelitis (VO) in France: analysis of hospital-discharge data 2002-2003. Epidemiol Infect. 2008. 136:653–660.

2. Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008. 56:401–412.
3. Karadimas EJ, Bunger C, Lindblad BE, Hansen ES, Høy K, Helmig P, Kannerup AS, Niedermann B. Spondylodiscitis. a retrospective study of 163 patients. Acta Orthop. 2008. 79:650–659.
4. Kim SY, Hong SJ, Lee CY, Chung KB, Park CM. Tuberculous spondylitis vs pyogenic spondylitis: focusing on the discriminative MR findings for differentiation. J Korean Radiol Soc. 2007. 56:183–189.
5. Koo KH, Lee HJ, Chang BS, Yeom JS, Park KW, Lee CK. Differential diagnosis between tuberculous spondylitis and pyogenic spondylitis. J Korean Soc Spine Surg. 2009. 16:112–121.
6. Lee KY, Sohn SK, Hwang KS. Comparison of pyogenic and tuberculous spondylitis. J Korean Soc Spine Surg. 1999. 6:443–450.
7. Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A. Pyogenic vertebral osteomyelitis: a systematic review of clinical characteristics. Semin Arthritis Rheum. 2009. 39:10–17.
8. Zimmerli W. Clinical practice. Vertebral osteomyelitis. N Engl J Med. 2010. 362:1022–1029.
9. Colmenero JD, Jiménez-Mejías ME, Sánchez-Lora FJ, Reguera JM, Palomino-Nicás J, Martos F, García de las Heras J, Pachón J. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: a descriptive and comparative study of 219 cases. Ann Rheum Dis. 1997. 56:709–715.
10. McHenry MC, Easley KA, Locker GA. Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis. 2002. 34:1342–1350.
11. Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev. 2000. 23:175–204.
12. Govender S. Spinal infections. J Bone Joint Surg Br. 2005. 87:1454–1458.
13. Lee DG, Park KB, Kang DH, Hwang SH, Jung JM, Han JW. A clinical analysis of surgical treatment for spontaneous spinal infection. J Korean Neurosurg Soc. 2007. 42:317–325.
14. Park WW, Ahn SJ, Lee JS, Kim TH. Comparison of two surgeries in active thoracolumbar tuberculous spondylitis: one stage anterior debridement with anterior instrumentation and two stage operation of anterior debridement and posterior instrumentation. J Korean Soc Spine Surg. 2003. 10:146–153.
15. Chang MC, Wu HT, Lee CH, Liu CL, Chen TH. Tuberculous spondylitis and pyogenic spondylitis: comparative magnetic resonance imaging features. Spine (Phila Pa 1976). 2006. 31:782–788.
16. Buchelt M, Lack W, Kutschera HP, Katterschafka T, Kiss H, Schneider B, Kotz R. Comparison of tuberculous and pyogenic spondylitis. An analysis of 122 cases. Clin Orthop Relat Res. 1993. 296:192–199.
17. Osenbach RK, Hitchon PW, Menezes AH. Diagnosis and management of pyogenic vertebral osteomyelitis in adults. Surg Neurol. 1990. 33:266–275.
18. Perronne C, Saba J, Behloul Z, Salmon-Céron D, Leport C, Vildé JL, Kahn MF. Pyogenic and tuberculous spondylodiskitis (vertebral osteomyelitis) in 80 adult patients. Clin Infect Dis. 1994. 19:746–750.
19. Khan IA, Vaccaro AR, Zlotolow DA. Management of vertebral diskitis and osteomyelitis. Orthopedics. 1999. 22:758–765.
20. Lam KS, Webb JK. Discitis. Hosp Med. 2004. 65:280–286.
21. Wirtz DC, Genius I, Wildberger JE, Adam G, Zilkens KW, Niethard FU. Diagnostic and therapeutic management of lumbar and thoracic spondylodiscitis--an evaluation of 59 cases. Arch Orthop Trauma Surg. 2000. 120:245–251.
22. Hadjipavlou AG, Mader JT, Necessary JT, Muffoletto AJ. Hematogenous pyogenic spinal infections and their surgical management. Spine (Phila Pa 1976). 2000. 25:1668–1679.
23. Roblot F, Besnier JM, Juhel L, Vidal C, Ragot S, Bastides F, Le Moal G, Godet C, Mulleman D, Azaïs I, Becq-Giraudon B, Choutet P. Optimal duration of antibiotic therapy in vertebral osteomyelitis. Semin Arthritis Rheum. 2007. 36:269–277.
24. Livorsi DJ, Daver NG, Atmar RL, Shelburne SA, White AC Jr, Musher DM. Outcomes of treatment for hematogenous Staphylococcus aureus vertebral osteomyelitis in the MRSA ERA. J Infect. 2008. 57:128–131.
25. Sakkas LI, Davas EM, Kapsalaki E, Boulbou M, Makaritsis K, Alexiou I, Tsikrikas T, Stathakis N. Hematogenous spinal infection in central Greece. Spine (Phila Pa 1976). 2009. 34:E513–E518.
26. Butler JS, Shelly MJ, Timlin M, Powderly WG, O'Byrne JM. Nontuberculous pyogenic spinal infection in adults: a 12-year experience from a tertiary referral center. Spine (Phila Pa 1976). 2006. 31:2695–2700.
27. Sampath P, Rigamonti D. Spinal epidural abscess: a review of epidemiology, diagnosis, and treatment. J Spinal Disord. 1999. 12:89–93.
28. Lu CH, Chang WN, Lui CC, Lee PY, Chang HW. Adult spinal epidural abscess: clinical features and prognostic factors. Clin Neurol Neurosurg. 2002. 104:306–310.
 XML Download
XML Download