

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
AIDS related malignancies have gradually decreased after the introduction of highly active antiretroviral therapy (HAART). Nevertheless, non-Hodgkin's lymphoma is still a major malignancy in resource limited countries that have difficulty supplying HAART, and same holds true for Korea. We report a case of non-Hodgkin's lymphoma involving the heart in a Korean AIDS patient, who presented with sudden arrhythmia and superior vena cava syndrome. He was diagnosed with AIDS in 2008, but refused to receive HAART. Immunohistologic findings were compatible diffuse large B cell lymphoma, and futher studies demonstrated involvement of the liver, adrenal gland, heart, and pericardiac space. HAART was initiated and non Hodgkin's lymphoma was successfully managed with intensive chemotherapy. This is the first cardiac involvement non Hodgkin's lymphoma in AIDS patients in Korea.
Figures and Tables
 | Figure 1(A) Chest CT scan taken on hospital day 1. Low attenuated lobulating mass in the right atrium with pericaridal effusion and left pleural effusion. (B) EKG taken hospital day 1. Sinus bradycardia 46 bpm with T wave inversion is seen in lead V1 to V3. (C) Echocardiograpy performed on hospital day 1. Mass (4.78 cm×2.55 cm) in the right atrium with pericardial effusion is observed.
|
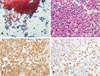 | Figure 2(A) Diffuse sheet of atypical large lymphoid cells are observed in PAP smear mixed with small reactive lymphocytes. (B) Atypical large lymphoid cells show nuclear hyperchromatism and prominent nucleoli on the CD cell block specimen. (C),(D) Strong immunopositivity for CD20 and increased MIB-1 index by immunohistochemical study.
|
 | Figure 3(A) EKG taken on hospital day 6 shows jucntional bradycardia with rate of 35 bpm, which was accompanied by dizziness. (B) Echocardiography performed on hospital day 6 revealed that the mass in right atrium has decreased from 4.78 cm×2.55 cm to 2.2 cm×1.5 cm after dexamethaxone treatment. (C) EKG taken on hospital day 22 demonstrates that the cardiac rhythm has normalized with its rate being 77 bpm. (D) Echocardiolgraphy performed on hospital day 22 shows that the right atrium mass has disappeared after the first EPOCH chemotherapy.
|
References
1. Engels EA, Biggar RJ, Hall HI, Cross H, Crutchfield A, Finch JL, Grigg R, Hylton T, Pawlish KS, McNeel TS, Goedert JJ. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer. 2008. 123:187–194.

2. Besson C, Goubar A, Gabarre J, Rozenbaum W, Pialoux G, Châtelet FP, Katlama C, Charlotte F, Dupont B, Brousse N, Huerre M, Mikol J, Camparo P, Mokhtari K, Tulliez M, Salmon-Céron D, Boué F, Costagliola D, Raphaël M. Changes in AIDS-related lymphoma since the era of highly active antiretroviral therapy. Blood. 2001. 98:2339–2344.
3. Bonnet F, Lewden C, May T, Heripret L, Jougla E, Bevilacqua S, Costagliola D, Salmon D, Chêne G, Morlat P. Malignancy-related causes of death in human immunodeficiency virus-infected patients in the era of highly active antiretroviral therapy. Cancer. 2004. 101:317–324.
4. Orem J, Otieno MW, Remick SC. AIDS-associated cancer in developing nations. Curr Opin Oncol. 2004. 16:468–476.
5. Seol YM, Song MG, Choi YJ, Lee SH, Kim SI, Chung JS, Kwak IS, Cho GJ, Lee H, Jung DS, Moon CS, Park JY. Trends in cancer risk among South Korean patients infected with Human Immunodeficiency Virus. Korean J Med. 2009. 76:554–563.
6. Levine AM, Sullivan-Halley J, Pike MC, Rarick MU, Loureiro C, Bernstein-Singer M, Willson E, Brynes R, Parker J, Rasheed S, Gill PS. Human immunodeficiency virus-related lymphoma. Prognostic factors predictive of survival. Cancer. 1991. 68:2466–2472.
7. Kaplan LD, Straus DJ, Testa MA, Von Roenn J, Dezube BJ, Cooley TP, Herndier B, Northfelt DW, Huang J, Tulpule A, Levine AM. National Institute of Allergy and Infectious Diseases AIDS Clinical Trials Group. Low-dose compared with standard-dose m-BACOD chemotherapy for non-Hodgkin's lymphoma associated with human immunodeficiency virus infection. N Engl J Med. 1997. 336:1641–1648.
8. Duong M, Dubois C, Buisson M, Eicher JC, Grappin M, Chavanet P, Portier H. Non-Hodgkin's lymphoma of the heart in patients infected with human immunodeficiency virus. Clin Cardiol. 1997. 20:497–502.
9. Butany J, Nair V, Naseemuddin A, Nair GM, Catton C, Yau T. Cardiac tumours: diagnosis and management. Lancet Oncol. 2005. 6:219–228.
10. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm Rep. 1992. 41:1–19.
11. Aboulafia DM, Pantanowitz L, Dezube BJ. AIDS-related non-Hodgkin lymphoma: still a problem in the era of HAART. AIDS Read. 2004. 14:605–617.
12. Gisselbrecht C, Oksenhendler E, Tirelli U, Lepage E, Gabarre J, Farcet JP, Gastaldi R, Coiffier B, Thyss A, Raphael M, Monfardini S. French-Italian cooperative group. Human immunodeficiency virus-related lymphoma treatment with intensive combination chemotherapy. Am J Med. 1993. 95:188–196.
13. Barbaro G, Barbarini G. HIV infection and cancer in the era of highly active antiretroviral therapy (Review). Oncol Rep. 2007. 17:1121–1126.
14. Choe PG, Song JS, Cho JH, Kim SH, Park KH, Bang JH, Park WB, Kim HB, Kim DW, Kim TY, Heo DS, Oh MD, Kim NJ, Choe KW. Malignancies in patients with Human Immunodeficiency Virus infection in South Korea. Infect Chemother. 2006. 38:367–373.
15. Ezzat H, Filipenko D, Vickars L, Galbraith P, Li C, Murphy K, Montaner JS, Harris M, Hogg RS, Vercauteren S, Leger CS, Zypchen L, Leitch HA. Improved survival in HIV-associated diffuse large B-cell lymphoma with the addition of rituximab to chemotherapy in patients receiving highly active antiretroviral therapy. HIV Clin Trials. 2007. 8:132.
16. Antinori A, Cingolani A, Alba L, Ammassari A, Serraino D, Ciancio BC, Palmieri F, De Luca A, Larocca LM, Ruco L, Ippolito G, Cauda R. Better response to chemotherapy and prolonged survival in AIDS-related lymphomas responding to highly active antiretroviral therapy. AIDS. 2001. 15:1483–1491.
17. Vaccher E, Spina M, Talamini R, Zanetti M, di Gennaro G, Nasti G, Tavio M, Bernardi D, Simonelli C, Tirelli U. Improvement of systemic human immunodeficiency virus-related non-Hodgkin lymphoma outcome in the era of highly active antiretroviral therapy. Clin Infect Dis. 2003. 37:1556–1564.
18. Choi HS, Choi K, Oh SJ, Yeom JS, Cho EY, Lee SS. A case of small bowel Burkitt's lymphoma in AIDS patient. Korean J Med. 2004. 66:543–548.
19. Sackoff JE, Hanna DB, Pfeiffer MR, Torian LV. Causes of death among persons with AIDS in the era of highly active antiretroviral therapy: New York city. Ann Intern Med. 2006. 145:397–406.
 XML Download
XML Download