

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Nontuberculous mycobacteria (NTM) is widely present in environment but it rarely causes infections in human. However, when NTM infects humans, it can cause pulmonary infection, lymphadenitis, skin infections, disseminated infection, etc. Of theses disease, pulmonary infection occurs most frequently while osteomyelitis is rare. In addition, osteomyelitis caused by Mycobacterium abscessus, an acid-fast bacillus classified as a pathogenic "rapid growing" NTM, is even rare and has never been reported in Korea. Although no consensus guidelines concerning the treatment of osteomyelitis caused by M. abscessus exist, prolonged antibiotics therapy in combination with surgical debridement is generally recommended. Herein, we reported the first case of knee joint osteomyelitis caused by M. abscessus in Korea. The patient experienced significant improvement after antibiotic treatment without recourse to surgery.
Figures and Tables
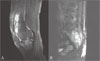 | Figure 1Magnetic resonance imaging (sagittal section) of (A) affected knee and (B) lumbar spine on initial visit. It shows high signal intensity on T2-weighted image.
|
 | Figure 2Magnetic resonance imaging (sagittal section) of (A) affected knee and (B) lumbar spine after 8 month's therapy of antibiotics. It shows some improvement of osteomyelitis at the lumbosacral bodies and regression of epidural abscesses.
|
Table 1
Result of antimicrobial susceptibity test of M. abscessus isolate from case patient

MIC, minimum inhibitory concentration; S, Susceptible; I, Intermediate; R, Resistant.
aIn general, sensitivity of imipenem is not reported in M. abscessus due to lack of reproducibility and for being prone to misinterpretation.
bIn general, MIC range of Moxifloxacin is reported instead of sensitivity in M. abscessus due to limited clinical data in treatment of M. abscessus using moxifloxacin.
![]()
References
1. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, Holland SM, Horsburgh R, Huitt G, Iademarco MF, Iseman M, Olivier K, Ruoss S, von Reyn CF, Wallace RJ Jr, Winthrop K. ATS Mycobacterial Diseases Subcommittee. American Thoracic Society. Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007. 175:367–416.

2. Medical Section of the American Lung Association. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Am J Respir Crit Care Med. 1997. 156:S1–S25.
3. Subcommittee of the Joint Tuberculosis Committee of the British Thoracic Society. Management of opportunist mycobacterial infections: Joint Tuberculosis Committee Guidelines 1999. Thorax. 2000. 55:210–218.
4. Jo KU, Park SJ, Hong SC, Oh YM, Lee SD, Kim WS, Kim DS, Kim WD, Shim TS. Long-term outcome of treatment of Mycobacterium abscessus pulmonary disease. Tuberc Respir Dis. 2007. 62:98–104.
5. Koh WJ, Kwon OJ. Diagnosis and treatment of nontuberculous mycobacterial lung disease. Korean J Med. 2008. 74:120–131.
6. Koh WJ, Kwon OJ, Yu CM, Jeon KM, Suh GY, Chung MP, Kim HJ, Han SW, Park SY, Lee NY. Recovery rate of nontuberculous mycobacteria from acid-fast-bacilli smear-positive sputum specimens. Tuberc Respir Dis. 2003. 54:22–32.
7. Phillips MS, von Reyn CF. Nosocomial infections due to nontuberculous mycobacteria. Clin Infect Dis. 2001. 33:1363–1374.
8. O'Brien DP, Currie BJ, Krause VL. Nontuberculous mycobacterial disease in northern Australia: a case series and review of the literature. Clin Infect Dis. 2000. 31:958–968.
9. Ryu SW, Lee CK, Heo J, Shin KS, Kim JS, Bae SY, Chang EA, Suh IB, Kim YK, Lee KN. A Case of knee Joint infection by Mycobacterium abscessus. Korean J Clin Pathol. 2001. 21:371–376.
10. Brown-Elliott BA, Wallace RJ Jr. Clinical and taxonomic status of pathogenic nonpigmented or late-pigmenting rapidly growing mycobacteria. Clin Microbiol Rev. 2002. 15:716–746.
11. Moore M, Frerichs JB. An unusual acid-fast infection of the knee with subcutaneous, abscess-like lesions of the gluteal region; report of a case with a study of the organism, Mycobacterium abscessus, n. sp. J Invest Dermatol. 1953. 20:133–169.
12. Galil K, Miller LA, Yakrus MA, Wallace RJ Jr, Mosley DG, England B, Huitt G, McNeil MM, Perkins BA. Abscesses due to Mycobacterium abscessus linked to injection of unapproved alternative medication. Emerg Infect Dis. 1999. 5:681–687.
13. Byun YS, Kim HT, Chang SA, Lee SR, Hwang DH, Kim SH. Iatrogenic spinal infection after injection therapy in spine. J Korean Soc Spine Surg. 2006. 13:299–305.
14. Bar T, Mishal J, Lewkowicz A, Nahlieli O. Osteomyelitis of the mandible due to Mycobacterium abscessus: a case report. J Oral Maxillofac Surg. 2005. 63:841–844.
15. Petitjean G, Fluckiger U, Schären S, Laifer G. Vertebral osteomyelitis caused by non-tuberculous mycobacteria. Clin Microbiol Infect. 2004. 10:951–953.
 XML Download
XML Download