

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The computer-aided design and computer-aided manufacturing (CAD/CAM) technologies have recently been applied to fabricate dental prostheses. The use of additive manufacturing (AM) process, often referred to as three-dimensional (3D) printing, for the fabrication of dental prostheses continues to obtain greater acceptance exhibiting some advantages over subtractive milling system which would lead to rapid wear of milling tools and increased cost.12 In addition, due to its flexibility in terms of designs and materials, AM technique has various applications in dentistry including dental prostheses,2 non-biological models for a pre-operative treatment planning and surgical training,3 dental implants,4 and tissue scaffold,5 etc. One of the most effective additive manufacturing techniques for metal is direct metal laser sintering (DMLS). This process can be used to build specialized components out of almost any metal alloy. The DMLS gradually builds up a 3D object through a series of very thin layers with laser sintering.6 Cobalt-chromium (Co-Cr) is widely used for DMLS manufacturing technique as substructures of dental prostheses exhibiting lower cost than precious metals, satisfactory bond strength to porcelain, good mechanical properties, and corrosion resistance.7
The success of implant therapy involves optimal esthetics as well as biomechanical function. Implant rehabilitation in the edentulous maxilla could be more complex than in the edentulous mandible. A great amount of horizontal atrophy following tooth extractions in the anterior part of the maxilla,8 limited vertical space for the implant placement,9 and poor bony quality9 could be critical factors in the edentulous maxilla. Zirconia is very tough, durable, and biocompatible in nature.10 Improved translucency and coloring techniques give them a better natural look11 and thus, full-contour monolithic zirconia crowns are increasingly obtaining popularity, making them a restorative option in the anterior as well as the posterior region.
The aims of this case report were to describe the successful outcome of an implant-supported fixed dental prosthesis in the edentulous maxilla that involved the use of a Co-Cr framework by using the DMLS technology and CAD/CAM monolithic zirconia crowns, and to describe its clinical implications.
Case Report
A 51-year-old woman presented to One-stop Specialty Center at Seoul National University Dental Hospital, Seoul, Korea. Her chief complaint was “all my upper teeth are mobile and are bothering me while chewing”. The clinical and radiographic examinations revealed grade 3 mobility12 of all upper teeth and severe bone loss in the entire maxillary arch (Fig. 1). Possible treatment options were offered to the patient, including extraction of all maxillary teeth, followed by the restoration either with a conventional complete denture or with an implant-supported restoration. The patient was given the information and we decided to determine the best treatment plan with the patient after post-extraction healing. All maxillary teeth were extracted and the interim denture was delivered.
After a healing period of 3 months,13 extra-oral and intra-oral examinations were assessed. Lip support was evaluated with and without the interim denture in place. The loss of lip support was identified without the denture due to moderate bone resorption of the anterior maxilla. There was a discrepancy between expected anterior teeth position and alveolar ridge. Since the patient was a middle school teacher, she was afraid of falling down of her denture during speech. She also had slurred speech and felt uncomfortable with her interim denture. She desired a fixed prosthesis which would be secure and feel like natural teeth. The patient had a moderate smile line14 with a long upper lip.
The intraoral examination revealed a loss of interdental papillae, thin mucosa in the pre-maxilla, and relatively thick mucosa in the posterior maxilla. The patient's upper arch had an ovoid form. Available inter-arch space was measured with the diagnostic mounted casts and the space between the maxillary edentulous ridge and the opposing occlusal plane was 13 – 15 mm. Considering the amount of alveolar bone resorption, the patient was told that gingiva-colored porcelain would be required to compensate tissue loss. The patients had relatively opaque teeth in the mandibular dentition. Based on a careful assessment of the extra-oral, intra-oral examinations, interarch space, translucency of the opposing dentition, and the patient's demands, CAD/CAM monolithic zirconia crowns bonded on the Co-Cr framework produced by using the DMLS technique was planned as a definitive prosthesis.
From the CT scan, the amount of bone available for the placement of implants and bone quality were evaluated. With a periodontist, the number of implants to be placed and the location of the implants were planned, and implants (4.0 × 10 mm USIII SA, Osstem Implant Co., Busan, Korea) were then placed into the planned sites using a surgical guide, a duplicate of the interim denture. Including two implants in the incisor region, eight implants with adequate anteriorposterior distribution allowed biomechanically stable prosthetic design.15
The patient healed adequately and at 5 months, the restoration process was begun. An open tray impression was taken with regular-body polyvinyl siloxane (Imprint II Garant, 3M ESPE, St. Paul, MN, USA). A wax occlusal rim in which temporary abutments were positioned to stabilize the wax rim was fabricated and the bite registration was carried out intra-orally. CAD/CAM-milled titanium abutments were fabricated based on the CAD data. A one-piece verification stent on the abutments was made with pattern resin (Duralay, Reliance Dental, Worth, IL, USA) and passive fit of the stent was checked intra-orally. A new intra-oral occlusal record was taken on the stent (Fig. 2).
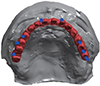
Overall appearance and occlusion were evaluated with the teeth in wax form. We have the patient make the ‘F’ sound to establish the proper incisal edge position. The inclination of central incisors was determined to provide adequate lip support. Eight abutments were digitally scanned with a 3D scanner (D700, 3Shape, Düsseldorf, Germany) and the 3D design of a framework was obtained with software (EOS RP Tools, EOS, Krailling, Germany). The framework was sintered from Co-Cr metal powder (EOS Co-Cr SP2, EOS, Krailling, Germany) sized 20 µm thickness in a DMLS system (M270, EOS, Krailling, Germany) at a scan speed of 7.0 m/s. Since the screw access holes were in non-esthetic locations, a cement-retained onepiece framework was fabricated to splint the implants together (Fig. 3), providing more passive fit than screw-retained.16 Thereafter, a post-processing heat treatment was applied at 750℃ for one hour to relieve thermal stress. The Co-Cr framework was covered with colored porcelains (Vintage Halo, Shofu, Kyoto, Japan).
At the framework try-in appointment, the framework was placed onto the abutments in the patient's mouth and checked for the fit and the passivity. Fourteen individual monolithic zirconia crowns (NexxZr T, Sagemax Bioceramics Inc., Federal Way, WA, USA) were constructed and tried them intra-orally before final characterization and glazing. At this appointment, definitive evaluations of occlusion, facial support, optimal phonetics, smile line, and esthetics were evaluated.
Each crowns were adhesively cemented on the framework with a resin cement (Panavia F 2.0, Kuraray Noritake Dental Inc., Tokyo, Japan) by using a stereomicroscope (S300-II, Ziecor, Sendai, Japan) extra-orally (Fig. 4). The abutments were connected with 30 Ncm torque, respectively and then, the one-piece framework with monolithic zirconia crowns was cemented on the abutments with a non-eugenol temporary resin cement (Premier implant cement, Premier Dental, Plymouth Meeting, PA, USA). Centric holding contacts were provided without interference to excursions. The use of a Co-Cr framework with gingiva-colored porcelains improved the lip and facial support. Post-delivery instructions were given at the time of delivery. The patient felt comfortable and was pleased with the esthetic outcomes of the prosthesis (Fig. 5). The patient was further evaluated at 2 weeks and at 6 months (Fig. 6), and the patient adapted well to her prosthesis. The prosthesis exhibited good stability and performance.
Discussion
The additive manufacturing technique is gaining popularity as it is capable of accurate reproduction of details and the fabrication of complex shapes from the CAD data.12 Several studies on the marginal adaptations of Co-Cr frameworks by using the DMLS method have been investigated. One study reported that DMLS-fabricated Co-Cr crowns displayed significantly smaller marginal gaps than conventional cast Co-Cr crowns.17 Likewise, in another study, the smaller values of fits were noted in the DMLS-fabricated Co-Cr three unit fixed dental prostheses (FDPs) than those of conventional or CAD/CAM-fabricated FDPs.18 On the contrary, Tamac et al.' s study showed significantly higher values of marginal and internal gaps for DMLS-fabricated Co-Cr crowns compared to CAD/CAM or traditional casting crowns.19 Although different measurement protocols were conducted in those studies, the obtained marginal gaps ranged from 84.0 µm to 102.9 µm which would be clinically acceptable.20 Therefore, DMLS-fabricated Co-Cr frameworks could be suitable for clinical applications in terms of the marginal adaptation. However, further researches to reduce the marginal discrepancies of dental prostheses by using DMLS systems should be performed.
Attaining a passive fit of the long-span implant retained prosthesis could be a significant factor for the success of implant restorations. The framework misfit would induce stress on the abutments and their respective implants, resulting in biomechanical implant failures. Kan et al. evaluated vertical misfits of cement-retained implant-supported 3-unit FDPs fabricated by the conventional casting procedure.21 The casting structures presented roughened textures and certain amount of distortions were detected due to the changes in volume during the investing and casting processes. Therefore, the DMLS additive manufacturing could be an efficient method for the fabrication of longspan prostheses minimizing the problem of distortion, since it is possible to build objects directly from CAD files, layer by layer, through local melting of metal powders with a layer thickness up to 25 µm.2 In addition, utilizing the DMLS system allows for the creation of complex shaped three dimensional structures with no need for tooling and thus, increases productivity.2 DMLS technique enables direct production of larger and more complex metal structures without wasting time and cost compared to CAD/CAM milling system. In addition, with DMLS prototyping, no tooling is required. However, DMLS system requires additional post processing in order to retain proper shape and tolerance.
Conclusion
Additive manufacturing appears to be promising for the use in dental restorations. Clinical success of the implant-supported fixed complete arch dental prostheses would depend on their reliable accuracy and passive fit. In this case report, a one-piece framework by using the DMLS technology and CAD/CAM monolithic zirconia crowns cemented on the framework in the edentulous maxilla exhibited a stable passivity as well as satisfactory esthetics with reduced manufacturing time and cost.





 XML Download
XML Download