

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Amelogenesis imperfecta characterized as abnormally formed enamel is caused by a defect of unique group of genes. Patients affected by this disease might have difficulties in social and psychological aspects due to non-esthetic teeth as well as functional problems caused by enamel detachment and tooth wear from their early ages. Adult patients with amelogenesis imperfecta can be treated with full-mouth restorations, which make functional and esthetic rehabilitations of severely worn tooth. However, the anterior open bite and lack of occlusal clearance for posterior teeth restorations due to compensatory extrusion are the intervening factors in the prosthetic treatment. Therefore, the determination of anterior tooth lengths, vertical dimension, and anterior guidance should be set carefully. Recently, computer-aided design and computer-aided manufacturing (CAD/CAM) techniques help systematic approaches and enable dentists to reduce time-consuming procedures in the diagnosis and treatment of full-mouth rehabilitation. This case report demonstrates the successful full mouth rehabilitation using a CAD/CAM system in a young adult patient with amelogenesis imperfecta and anterior open bite.
Figures and Tables
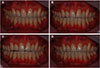
Fig. 1
Preoperative intraoral view showing generalized tooth wear and anterior open bite. (A) Occlusal view of maxilla, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Occlusal view of mandible.





Fig. 6
1st provisional restorations. Approximate occlusal plane and tooth contour, patient's adaptation to occlusal change, disappearance of hypersensitivity, and occlusal clearance for posterior restoration were evaluated through 1st provisional restorations. (A) Extraoral photo, (B) Intraoral photo.

Fig. 7
CAD/CAM procedure for 2nd provisional prostheses. (A) Incisal edges and occlusal plane evaluation on virtual model, (B) Frontal view of maxillary crowns.




References
1. DeSort KD. Amelogenesis imperfecta: The genetics, classification, and treatment. J Prosthet Dent. 1983; 49:786–792.

2. Ayers KM, Drummond BK, Harding WJ, Salis SG, Liston PN. Amelogenesis imperfecta-multidisciplinary management from eruption to adulthood. Review and case report. N Z Dent J. 2004; 100:101–104.
3. Rajesh P, Prasad M, Haldal S. Full mouth rehabilitation of a patient with amelogenesis imperfecta: a case report. J Int Oral Health. 2014; 6:76–79.
4. Witkop CJ, Sauk JJ. Heritable defects of enamel. In : Stewart RE, Prescott GH, editors. Oral facial genetics. St. Louis: C.V. Mosby;1976. p. 151–226.
5. Rowley R, Hill FJ, Winter GB. An investigation of the association between anterior open-bite and amelogenesis imperfecta. Am J Orthod. 1982; 81:229–235.
6. Hoppenreijs TJ, Voorsmit RA, Freihofer HP, van't Hof MA. Open bite deformity in amelogenesis imperfecta. Part 2: Le Fort I osteotomies and treatment results. J Craniomaxillofac Surg. 1998; 26:286–293.
7. Kostoulas I, Kourtis S, Andritsakis D, Doukoudakis A. Functional and esthetic rehabilitation in amelogenesis imperfecta with allceramic restorations: a case report. Quintessence Int. 2005; 36:329–338.
8. Yip HK, Smales RJ. Oral rehabilitation of young adults with amelogenesis imperfecta. Int J Prosthodont. 2003; 16:345–349.
9. Binkley TK, Binkley CJ. A practical approach to full mouth rehabilitation. J Prosthet Dent. 1987; 57:261–266.
10. Kordass B, Ruge S, Ratzmann A, Hugger A. Current technologies for functional diagnostics and CAD/CAM. Int J Comput Dent. 2013; 16:163–171.
11. Reich S. Tooth-colored CAD/CAM monolithic restorations. Int J Comput Dent. 2015; 18:131–146.
12. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology. 2nd ed. Philadelphia: WB Sanders Co.;2002. p. 96.
13. Sciasci P, Abi-Rached FO, Adabo GL, Baldissara P, Fonseca RG. Effect of surface treatments on the shear bond strength of luting cements to Y-TZP ceramic. J Prosthet Dent. 2015; 113:212–219.
14. Ozcan M. Evaluation of alternative intra-oral repair techniques for fractured ceramic-fused-to-metal restorations. J Oral Rehabil. 2003; 30:194–203.
15. Al-Amleh B, Lyons K, Swain M. Clinical trials in zirconia: a systematic review. J Oral Rehabil. 2010; 37:641–652.
16. Palacios RP, Johnson GH, Phillips KM, Raigrodski AJ. Retention of zirconium oxide ceramic crowns with three types of cement. J Prosthet Dent. 2006; 96:104–114.
17. Thompson JY, Stoner BR, Piascik JR, Smith R. Adhesion/cementation to zirconia and other non-silicate ceramics: where are we now? Dent Mater. 2011; 27:71–82.
18. Melo RM, Souza RO, Dursun E, Monteiro EB, Valandro LF, Bottino MA. Surface treatments of zirconia to enhance bonding durability. Oper Dent. 2015; 40:636–643.
19. Ozcan M, Cura C, Valandro LF. Early bond strength of two resin cements to Y-TZP ceramic using MPS or MPS/4-META silanes. Odontology. 2011; 99:62–67.
20. Ozcan M, Kerkdijk S, Valandro LF. Comparison of resin cement adhesion to Y-TZP ceramic following manufacturers' instructions of the cements only. Clin Oral Investig. 2008; 12:279–282.
 XML Download
XML Download