

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Donggyu Lee , Jeongkyung Kang
, Jeongkyung Kang
, Jeongkyung Kang
Abstract
Maxillofacial defect comes from congenital defect, trauma and surgical resection. Patients with intraoral defect are commonly related to maxillary defect and they need prosthetic rehabilitation. Functional reconstruction of partially edentulous mandible has many limitations. However, if both condyles are intact, maxillofacial prosthesis using partial denture give competent results. In this case, a patient of 58 year-old male has a defect on palate and left mandibular posterior teeth from gunshot. The maxillary defect of this patient is Class IV according to Aramany classification and the mandibular one is Type V according to Cantor and Curtis classification. For retention of the obturator, remaining teeth are fully utilized and artificial teeth are arranged harmoniously to provide stable occlusion. Mandibular RPD covered limited range of deformed soft tissue derived from mandibular resection surgery. With these treatments, the patient in this case showed improvements in mastication, swallowing and speech.
Figures and Tables

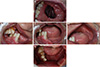 | Fig. 2Initial intraoral photographs. (A) Maxillary occlusal view, (B) Lateral view (right), (C) Frontal view, (D) Lateral view (right) (E) Mandibular occlusal view.
|





References
1. Keyf F. Obturator prostheses for hemimaxillectomy patients. J Oral Rehabil. 2001; 28:821–829.

2. Beumer J, Curtis TA, Marunick M. Maxillofacial rehabilitation: Prosthodontic and surgical considerations. St. Louis, MO: Ishiyaku EuroAmerica, Inc.;1996.
3. Aramany MA. Basic principles of obturator design for partially edentulous patients. Part I: classification. J Prosthet Dent. 1978; 40:554–557.
4. Aramany MA. Basic principles of obturator design for partially edentulous patients. Part II: design principles. J Prosthet Dent. 1978; 40:656–662.
5. Firtell DN, Curtis TA. Removable partial denture design for the mandibular resection patient. J Prosthet Dent. 1982; 48:437–443.
6. Shifman A, Lepley JB. Prosthodontic management of postsurgical soft tissue deformities associated with marginal mandibulectomy. Part I: Loss of the vestibule. J Prosthet Dent. 1982; 48:178–183.
7. Cantor R, Curtis TA. Prosthetic management of edentulous mandibulectomy patients. I. Anatomic, physiologic, and psychologic considerations. J Prosthet Dent. 1971; 25:446–457.
8. Parr GR, Tharp GE, Rahn AO. Prosthodontic principles in the framework design of maxillary obturator prostheses. 1989. J Prosthet Dent. 2005; 93:405–411.
9. Chalian V, Drane J, Standish S. Maxillofacial prosthetics. Williams & Wilkins Co.: Baltimore;1971. p. 133–148.
 XML Download
XML Download