

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bone avascular necrosis (AVN) is a common late complication after kidney transplantation (KT), with a reported incidence of 3% to 30%(1234). AVN, a pathological condition defined as death of all cellular elements and progressive destruction of the bone, occurs because of bone vasculature disruption, death of osteocytes and fat cells, and bone architecture alterations(56). Generally, various factors such as corticosteroid administration, alcohol use, smoking, radiation, hyperlipidemia, thrombophlebitis, and intravascular coagulation have been proposed as risk factors for AVN throughout the population(789). Joint pain radiating to buttocks, thighs, or knees while the patient bears their weight on the affected joint is the first and typical symptom of AVN(10). Pain is presumed to be related to bone marrow edema that can be observed using magnetic resonance imaging in early-stage AVN(11).
KT has been reported as a prominent AVN risk factor. Although corticosteroid treatment after transplantation is frequently predicted as the main contributor for AVN after KT, several studies also reported other risk factors in addition to steroid regimen in relation to AVN development(312131416). A study reported that higher cumulative steroid dose, high blood urea nitrogen levels, immunosuppressive drug treatment, and impaired blood flow caused by arterial ischemia and/or venous thrombosis were potential risk factors for AVN(12). A recent report indicated that steroid administration within 2 weeks after KT exhibited a dose-dependent relationship with AVN development(3). Treatment with calcineurin inhibitors, mycophenolate mofetil, cyclosporine, or sirolimus, acute rejection, and female sex were also suggested as risk factors for AVN development after transplantation(13141516).
Recently, KTs across immunologic barriers, such as flow-cytometry cross matching (FCXM)-positive KT and ABO-incompatible KT, have been increasingly performed. Under such circumstances, use of higher doses of immunosuppressive drugs and additive treatment for pretransplant desensitization are expected based on immunological risks. Additionally, the number of patients receiving steroid pulse treatments due to acute rejection are expected to increase. In this retrospective study, we determined the incidence of AVN after KT and investigated the risk factors associated with AVN development with regard to recent transplantation trends.
MATERIALS AND METHODS
This was a retrospective observational study that included data from patient medical record reviews. The study protocol was approved by the Institutional Review Board of Asan Medical Center (2014-0776) without a written informed consent. Totally, 1,570 consecutive patients that underwent living-donor KT at Asan Medical Center between January 2009 and July 2016 were included in the study after the exclusion of 486 patients who underwent cadaveric donor KT during the study period. Patient information included age, body mass index, sex, and past medical history as well as immunologic risk factors including panel-reactive antibody, human leukocyte antigen mismatches, and FCXM. Rejection-free graft survival was defined as the time taken from transplantation to acute rejection and was pathologically diagnosed according to the Banff criteria(17). Furthermore, data on rejection management, particularly steroid pulse treatment, were recorded.
The immunosuppressive regimen at our institution comprised induction with an interleukin-2 antagonist (basiliximab, 20 mg) on days 0 and 4, which was administered to all but 65 patients who received rabbit antithymocyte globulin (4.5 mg/kg), together with a calcineurin inhibitor (tacrolimus or cyclosporine), mycophenolic acid, and a corticosteroid (methylprednisolone [mPD]). Patients with ABO-incompatible or FCXM-positive KT as well as highly sensitized individuals were administered anti-CD20 antibody (rituximab) before transplantation. Target trough levels for tacrolimus and cyclosporine were 6 to 8 ng/mL and 100 to 150 µg/L, respectively, during the early postoperative period, and were lower at 3 to 6 ng/mL and 50 to 100 µg/L, respectively, after 1 year. Patients were administered 1,500 mg mycophenolate mofetil or 1,080 mg mycophenolic acid daily as an anti-metabolite agent. Rituximab dose (200 or 500 mg) was determined based on the patient's pretransplant ABO isoagglutinin titers or immunologic risks.
According to the steroid protocol at our institution, 500 mg mPD was intravenously administered during surgery. After intravenous administration of 250 mg mPD on postoperative day (POD) 1 and 125 mg mPD from POD 2 to 3, the oral mPD dose was gradually decreased to 80, 80, 64, 64, 48, 48, 24, 24, and 16 mg daily until POD 12. A 16-mg maintenance mPD dose was attained until POD 30. Recipients received 12 mg/day mPD from POD 31 to POD 60, 10 mg/day mPD from POD 61 to POD 90, 8 mg/day mPD from POD 91 to POD 180, and 6 mg/day mPD from POD 181 to POD 365. A 4-mg mPD maintenance dose was attained 1 year after transplant. Forty-four patients (2.8%) were withdrawn from steroids within 1 week of transplantation and received only 995 mg mPD postoperatively, because they were enrolled in other clinical studies. Steroid pulse treatment was administered to patients who exhibited acute cellular rejection in biopsy specimens at an intravenous mPD dose of 500 to 4,000 mg.
AVN evaluation was conducted in patients with typical AVN symptoms such as movement restriction, pain, or disturbance in walking. AVN was diagnosed using magnetic resonance imaging findings(418) and clinical diagnosis according to current guidelines, and the diagnosis was conducted by orthopedic surgeons at our institution(19). The AVN treatment plan was determined according to the AVN stage and symptom severity. Although patients with association of research circulation osseous (ARCO) grade I and II AVN were treated with conservative treatment and steroid dose reduction, surgical treatment was performed in those with ARCO grade III and IV AVN(19).
Categorical variables presented as numbers with percentages were analyzed using the chi-square test. Comparisons of continuous variables, presented as mean±standard deviation, were performed using the Student t-test. Variables that were not normally distributed and were presented as medians (interquartile range) were analyzed using the Mann-Whitney U-test. The Cox proportional hazard regression model analysis was used for risk factor evaluation for AVN development. Variables with a P<0.1 by univariable analysis were analyzed using multivariable regression models. Rejection-free survival rate was measured using the Kaplan-Meier method and was compared using the log-rank test. All other statistical analyses were performed using the SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA), and P≤0.05 was considered statistically significant.
RESULTS
Of the 1,570 patients that underwent living-donor KT during the study interval, 33 (2.1%) developed AVN during a mean follow-up of 49.8±25.0 months. Demographics and clinical characteristics of the study cohort are presented in Table 1. There were significantly more female patients (P=0.02) and a significantly higher end-stage renal disease prevalence because of hypertension (P=0.01) among patients with AVN. Mean cumulative steroid dose during the last follow-up in patients without AVN (9,108±3,400 mg) was higher than that in patients with AVN (4,483±1,114 mg) until AVN occurrence (P<0.01). More patients in the AVN group (n=4, 12.1%) received steroid pulse treatment due to biopsy-proven rejection during the first 6 months after KT than patients without AVN did (n=68, 4.4%; P=0.04).
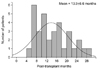
AVN was diagnosed at a mean of 13.9±6.6 months after KT (range, 5 to 29) (Fig. 1). The main AVN site was hip in 29 cases and knee in four cases. Totally, 14 patients (42.4%) were conservatively managed with steroid withdrawal, and 19 (57.6%) were surgically treated with total hip or knee arthroplasty (Table 2).
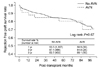
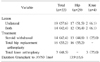
Univariate Cox proportional hazard regression analysis was conducted to evaluate risk factors associated with AVN development. Variables that showed significance with a cutoff P-value of 0.1 during univariate analysis were included in the multivariate analysis. Female gender (hazard ratio [HR], 2.29; 95% confidence interval [CI], 1.10 to 4.61; P=0.04) and steroid pulse treatment during the first 6 months after KT (HR, 2.31; 95% CI, 1.15 to 4.64; P=0.02) were significantly associated with AVN as revealed by multivariate analysis (Table 3). However, no significant difference in rejection-free graft survival rates between patients with AVN and without AVN were observed (P=0.67) (Fig. 2).
DISCUSSION
The incidence of symptomatic AVN in this retrospective study was 2.1% among patients that underwent KT. Additionally, female sex and steroid pulse treatment within 6 months after KT were independent risk factors for AVN development. The AVN incidence observed in the current study agrees with the reported 5.1% to 6% incidence among patients undergoing low-dose steroid treatment in recent studies(314). Shibatani et al.(20) and Saito et al.(3) reported that the steroid dose in the early postoperative period greatly impacted AVN development. Abbott et al.(13) reported that female recipients had a 1.3-fold (95% CI, 1.08 to 1.59; P=0.008) increase in odds for AVN development after more than a year of KT. However, cyclosporine use (in comparison with tacrolimus), which was reported as an independent risk factor for AVN development by Abbott et al.(13) was found to be insignificant in the current study.
Steroid usage, which is one of the most important causes of AVN(5), results in an increased intraosseous pressure and plasma fibrinogen level, decreased bone perfusion, fat embolization, and osteocyte apoptosis. Additionally, increased plasma fibrinogen levels significantly affect coagulation. Activation of intravascular coagulation has been suggested as an important event leading to ischemia(6), which causes disruption of bone vasculature and bone marrow, leading to ischemic necrosis of bony tissues and bone collapse(21).
Patients exposed to higher corticosteroid doses or those who underwent corticosteroid treatment for longer durations were considered to be at a higher risk for AVN(222). Although several studies revealed that cumulative corticosteroid doses were higher among patients with AVN(1423), the current study suggested that cumulative corticosteroid dose itself was not a risk factor for AVN development. Steroid usage is evidently a major cause of AVN after KT; however, not all recipients receiving steroids develop AVN. In the current study, the mean duration from KT to AVN development was 13.9±6.6 months (range, 5 to 29) in the AVN group. Serrano et al.(22) recently reported an AVN-free survival rate that was similar to that obtained in the current study and found that the recipients who did not develop AVN were exposed to higher cumulative doses for longer durations. Saito et al.(3) also reported a similar finding; particularly, a dose-dependent relationship between the total amount of steroids administered in the first 2 weeks after transplantation and AVN development was reported. A recent large, population-based study reported that AVN incidence was only 0.13% among patients treated with low-dose mPD of <15 to 20 mg/day(24). Although long-term, low-dose steroid replacement increases relative risk compared to no steroid treatment, repetitive high-dose steroid treatment within few months is predicted to greatly increase AVN risk, compared with prolonged low-dose treatment. In the current study, we compared the steroid dose within the first 6 months between patients with and without AVN because the earliest case of AVN was observed at 5 months after KT. In the present study, Steroid pulse therapy was considered a prominent risk factor for AVN development because the cumulative steroid dose during the first 6 months was similar between patients with and without AVN, except for patients who received steroid pulse treatment due to acute rejection. One patient who was included in the early steroid withdrawal group developed AVN because of steroid pulse treatment 3 months after transplantation. Although several studies reported that the osteonecrosis risk after KT was higher in patients who received cyclosporine for immunosuppression than in patients who received tacrolimus, those findings might be associated with the reduction in number of acute rejection episodes and the dose of pulse corticosteroid administration in patients receiving tacrolimus(1325). Pretransplant management of immunologic risks and maintenance immunosuppression treatment did not exhibit significant associations with AVN in our multivariate analysis.
The current study indicated that female sex was an independent risk factor for AVN development after KT. Although Abbott et al.(13) indicated female gender as one of the independent risk factors in their multivariate analysis, that finding was not a main feature of their study. Schulte and Beelen(15) reported that female sex significantly increased AVN risk after allogeneic hematopoietic stem cell transplantation and speculated that estrogen levels after transplantation could affect osteoclast and osteoblast activity. A study using a rat model for AVN reported that female rats were more severely affected because of sexual dimorphisms in the coagulation system(26). However, these studies did not clarify the exact mechanisms underlying sex-related differences in AVN occurrence. Further studies are warranted to explore the AVN pathogenesis in females.
The current study has several limitations. First, due to its retrospective nature, selection and information biases could not be ruled out. Second, the number of patients with AVN was relatively less. Third, AVN incidence might have been underestimated because only patients with symptomatic AVN underwent workup for AVN diagnosis. Finally, there might have been a lag time bias because diagnosis and treatment was performed only in patients with AVN symptoms.
CONCLUSION
Steroid pulse treatment within 6 months of KT and female sex were independent risk factors for AVN development. The results of the current study provide valuable information for physicians who manage recipients after KT. Although early steroid cessation and steroid avoidance should be considered in patients having low immunologic risk, proper desensitization and optimal immunosuppression to prevent acute rejection in highly sensitized patients can prevent AVN after KT. Further studies to determine sex-related differences in AVN development are warranted.


 XML Download
XML Download