

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Neisseria gonorrhoeae is the causative agent of gonorrhea, one of the most important sexually transmitted diseases and results in a wide range of diseases from asymptomatic infection to severe complications (1). Humans are the only hosts of this pathogen, and N. gonorrhoeae is always considered pathogenic even in asymptomatic patients. Most common type of infection is acute urethritis in men and endocervicitis in women, but up to 10% of men and many women may be asymptomatic. Most cases of untreated infections resolve spontaneously after several weeks, but severe complications such as pelvic inflammatory diseases and disseminated gonococcal infections may occur.
The prevalence of N. gonorrhoeae infection has decreased in many developed countries during the past few decades (2~4), but it is still high in many developing countries (5). According to the global estimation by the World Health Organization in 2011, 88 million new cases of gonococcal infections have been reported annually (6). The incidence of gonorrhea seemed to decrease in Korea recently according to the data from the Korean Centers for Disease Control and Prevention (7), but the data from the Korea Health Insurance Review and Assessment Service showed that gonorrhea is still prevalent and about 50,000 new cases have been reported annually during the late 2000s in Korea. Moreover, gonorrhea is very problematic in certain patient groups, such as adolescents in youth shelters (8). The prevalence of gonorrhea among university students was as low as 0.4% (9), but adolescents who had a sexual experience in youth shelters showed very high prevalence of 28% by polymerase chain reaction in 2004 in Korea (8).
Historically, gonorrhea has been a community-acquired disease and treated empirically at a primary-care hospital, and it has responded well to antimicrobial agents such as penicillin G and fluoroquinolones. However, the emergence of antimicrobial resistance in N. gonorrhoeae has compromised the treatment and control of the disease (10, 11). Due to the recent use of molecular diagnostic methods, the routine isolation and susceptibility testing of N. gonorrhoeae are performed rarely; therefore, it is hard to select optimal antibiotics in clinical settings. Therefore, surveillance program of antimicrobial resistance is required to establish the guideline for empirical treatment and control of gonococcal infection. The antimicrobial resistance of N. gonorrhoeae has been a serious problem in Korea (12~17). In this review, we discussed the current status of antimicrobial resistance of N. gonorrhoeae and of gonococcal infection in Korea.
Penicillin G, tetracycline, and fluoroquinolone
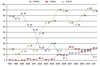
N. gonorrhoeae had been highly-susceptible to penicillin G. However, penicillin G lost its clinical usefulness rapidly since the clinical treatment failure of penicillin was reported in the 1950s in Korea (18). The annual rate of penicillin-susceptible N. gonorrhoeae collected during 1966-1975 varied from 7.7% to 26.7%, and the average rate of susceptible isolates during that period was only 12.1% in Korea (19). Resistance to penicillin G became more serious and no susceptible isolates were detected since the 1990s (12). Penicillin G resistance in N. gonorrhoeae is due to two different mechanisms: one is plasmid-mediated β-lactamase production (penicillinase-producing N. gonorrhoeae, PPNG) and another is changes in amino acid sequences in penicillin-binding protein (PBP) encoded by chromosomes (chromosomally-mediated penicillin-resistant N. gonorrhoeae, CMRNG). PPNG produces TEM-1 type β-lactamase, which confers high level resistance to penicillin G. The prevalence of PPNG increased steadily until the 1990s and remained high in many Asian countries as compared to most developed countries (20, 21). In Korea, the first case of PPNG was isolated in the US armed forces personnel, but he had a history of contract with the infection not in Korea but in South-East Asia where PPNG appeared for the first time (22). The true first case was isolated from 51-year-old housewife in Seoul in 1979, and it was supposed that PPNG occurred within Korea because both the patient and her husband had never traveled abroad (22). The proportion of PPNG steadily increased during the 1980s and 1990s and reached 84% in 1999 (Fig. 1), but decreased rapidly in the 2000s (12~17). The decline was also reported in other countries such as Hong Kong (23~25), but the exact cause was not known. Although the prevalence of PPNG decreased, all non-PPNG isolates was non-susceptible to penicillin G with elevated minimum inhibitory concentrations (MICs), indicating that penicillin G cannot be used to treat gonorrheal infection (14~17).
Tetracycline is another historical antimicrobial agent used to treat gonococcal infection but is no longer used. Tetracycline resistance arose from chromosomal mutations in tet, penB, and mtrR genes (low-level resistance) and acquisition of a conjugative tetM-containing plasmid (high-level tetracycline-resistant N. gonorrhoeae, TRNG) from other isolates (26). Although tetracycline is no longer prescribed as a treatment option, susceptibility to tetracycline can be tested routinely because the isolation trend of TRNG may be useful for epidemiologic studies. In Korea, tetracycline-susceptible isolates have not been detected since the early 1990s (12~17). The rate of TRNG was very low until 2004 (14), but the rate increased during the late 2000s (15~17) and finally reached to 22% in our 2011 study (Fig. 1), (unpublished data). The reason for the recent increase of TRNG is not clear, but the changes in epidemiology in gonococcal infection seemed to have happened and further investigation may be required.
Fluoroquinolones, such as ciprofloxacin and ofloxacin, started to be used for gonorrhea in the mid-1980s (27) and was one of the recommended drugs in the 1990s (28) because it had several advantages: it could be used orally in a single dose regimen and was highly concentrated in urine (29~31). However, frequent use of fluoroquinolones resulted in a wide spread of resistance (31, 32). In Korea, fluoroquinolone susceptibility was as high as 91% in 1992, but it rapidly decreased to 46% in 1996 (12). With continuous decrease of susceptible isolates, the resistance rate increased from 20% in 1997 (13) to 88% in 2011 in our present study (Fig. 1), (unpublished data). Fluoroquinolone resistance was mainly due to mutations in the target sites: the gyrA and parC genes. Most of the fluoroquinolone-resistant isolates had amino acid substitutions at the 91st and 95th positions in GyrA and a single substitution at the 86th or 87th position in ParC (14, 33). Accumulation of these mutations can lead to increased fluoroquinolone resistance. Because of rapid and progressive spread of resistance in clinical isolates, fluoroquinolones have not been recommended in the United States and Korea since 2007 (34~36). However, despite discontinuation of the use of fluoroquinolones, the prevalence of fluoroquinolone-resistant N. gonorrhoeae has not decreased and novel mutations in the gyrA and parC genes continued to be detected. This suggests slow but sustained evolution of the genes as a consequence of selection for fluoroquinolone resistance due to dual therapy for accompanying chlamydial infections. However, importation of strains with new QRDR substitutions is a more possible cause rather than de novo evolution.
Cephalosporin
Recently, cephalosporins have become one of the most active therapeutic choices for gonococcal infection. Ceftriaxone, cefotaxime, and cefixime are recommended by the Korean guideline for gonorrhea (34). Ceftriaxone is the predominantly used cephalosporin antimicrobial agent in gonococcal infection because of its high intrinsic activity against N. gonorrhoeae together with a long half-life and success in eradicating the organism from all sites of infection (37). Multi-drug resistance to penicillin G, tetracycline, and fluoroquinolone in N. gonorrhoeae led to a slight increase in the use of third-generation cephalosporins and spectinomycin in Korea (14). In 2002, only 9.5% of patients were treated with cephalosporins including parenteral ceftriaxone and oral cefixime. The rate increased to 30% in 2010. As cephalosporin is used more often, resistance to cephalosporin in N. gonorrhoeae has emerged (38~42). A recent Gonococcal Infection Surveillance Program in the U.S. showed an increasing trend of gonococcal isolates with elevated MICs of cefixime (≥0.25 µg/ml) from 0.2% in 2000 to 1.4% in 2010 and of ceftriaxone (≥0.125 µg/ml) from 0.1% in 2000 to 0.3% in 2010 (43). Sustained increase of MIC to near breakpoint within the susceptible range (MIC creep) hinders efficacy of cephalosporin antibiotics in gonorrheal treatment. Because the clinical efficacy of β-lactam antibiotics is related to the periods for which free drug concentration exceeds MIC (ƒT>MIC), increasing MIC decreases ƒT>MIC and clinical failure can arise. The current regimen of ceftriaxone (250 mg) and cefixme (400 mg) may be effective, but the MIC creep and resulting reduction of ƒT>MIC may be a cause of clinical failure in gonorrheal treatment with ceftriaxone and cefixime MICs of 0.125~0.25 µg/ml (44).
Ceftriaxone-resistant N. gonorrhoeae was not reported until 2011, but two cases of ceftriaxone-resistant isolates were reported in Japan (H041 strain, ceftriaxone MIC 2 µg/ml) and France (F89 strain, ceftriaxone MIC 2 µg/ml) in 2011 (45~47). The mechanism of resistance of these two strains was determined and seemed to be associated with novel penA mosaicism. In Korea, all isolates were susceptible to ceftriaxone in an annual successive study that was previously performed and supported by the Korea National Institute of Health. However, MIC creep was apparent (14): more than 32-fold difference was noted between the lowest and the highest MICs. The MIC range of ceftriaxone for N. gonorrhoeae in our previous study was ≤0.008~0.06 µg/ml during 1997 and 1999 (13), but the upper margin of MICs increased to 0.25 µg/ml near the breakpoint in isolates collected during the 2000s (14~17). The proportion of isolates inhibited by ≥0.06 µg/ml of ceftriaxone increased from less than 10% of the isolates from 1997-1999 (13) to 39% of the isolates from 2011 in our present study (unpublished data), and this meant 39% of N. gonorrhoeae isolated in Korea was not susceptible to ceftriaxone by the Australian guideline.
Ceftriaxone had a good activity in treating gonococcal infection, but it had to be given as an intramuscular injection that is locally painful and requires co-administration of a local anesthetic such as lidocaine. For this reason, the use of a number of oral cephalosporins was evaluated. Cefixime is one of the orally absorbed cephalosporins that is not only active against penicillin-resistant N. gonorrhoeae regardless of production of β-lactamase but also has pharmacokinetic activity suitable for single-dose administration. In a randomized unblinded multicenter study reported in 1991, a single dose of oral cefixime appeared to be as effective as ceftriaxone in the treatment of uncomplicated gonorrhea (48). Thereafter, cefixime and other oral cephalosporins such as cefuroxime axetil (49), ceftibuten (50), cefoperazone (51), cefdinir (52), cefpodoxime proxetil (53), and cefaclor (54) were used to treat gonococcal infection in many countries. However, an increasing number of treatment failures with oral cephalosporin regimens, especially with cefixime (55) and ceftibuten (42), were reported recently. Treatment failure with cefixime was reported first in 2001 in Japan, which was 10 years earlier than when ceftriaxone-resistant N. gonorrhoeae was reported in Japan in 2011. Cefixime-resistant N. gonorrhoeae disseminated widely and became common in Japan since 2001, and cefixime was no longer recommended as a treatment option in Japan (56~59). In Korea, cefixime non-susceptible N. gonorrhoeae (cefixime MIC, 0.5 µg/ml) was first isolated in 2004 (60), but there was no additional cefixime non-susceptible strain isolated in a successive study until 2010. This isolate had the identical genetic background and mechanism with isolates that were reported to be cefixime resistant in Japan in 2001.
The mechanism of resistance to cephalosporin has not been completely understood yet, but alterations in PBP2 seem to play an important role in cephalosporin resistance in N. gonorrhoeae. When the first cefixime-resistant N. gonorrhoeae was reported in Japan in 2001, it was suggested that mosaicism (Pattern X) in PBP2 encoded by the penA gene was associated with clinical failure and cefixime resistance because PBP2 was a main target of β-lactam antibiotics in N. gonorrhoeae (55, 61). The relationship between PBP2 alteration and cephalosporin susceptibility was supported by other studies (58, 61~63). In direct assays, mosaic PBP2 showed lower affinity with oral cephalosporins including cefixime and cefdinir than that of non-mosaic-structure PBP2, but affinity with ceftriaxone was not affected (61). In the modeling study, the A501V substitution in PBP2 also induced a conformational alteration of the β-lactam-binding pocket such as mosaic PBP2, making a major contribution to the reduced susceptibility to cephalosporin (58, 62, 63). A recent report on ceftriaxone-resistant N. gonorrhoeae showed that novel PBP2 mosaicism (46) (97.6% similarity with Pattern X) and A501P substitution (47) were also associated with ceftriaxone resistance. However, the mechanism of reduced susceptibility was not explained by penA mosaicism alone. N. gonorrhoeae with the mosaic PBP2 (Pattern X) showed variable MICs for cefixime from susceptible to resistant (56), and all N. gonorrhoeae with A501V were still susceptible to ceftriaxone despite elevated MICs, suggesting that other genetic changes may be needed to provoke resistance to cefixime. Reduced susceptibility of N. gonorrhoeae to cephalosporin was associated with diverse penA mutations, together with mtrR mutations (60). Mutations in the mrtR gene induced the derepression of an efflux pump repressor, and these mutations occurred almost always with an alteration in penB gene that encodes porin proteins (64) and in ponA gene that encodes PBP1. A mutation in recently identified pilQ gene (previously named penC) was also associated with reduced susceptibility of cephalosporins (65), but this mutation has not been observed in clinical settings. Sequential alterations of the penA, mtrR, penB, ponA,and pilQ genes have been shown to induce chromosomally mediated high-level resistance to penicillin and cephalosporin (60, 66).
Spectinomycin
Spectinomycin is another active antimicrobial agent that is cheap and active in uncomplicated gonorrhea (67). However, spectinomycin has to be administered as an intramuscular injection and can cause treatment failure in gonococcal pharyngitis (68). Although spectinomycin resistance had been reported in Korea in 1986 and 1993 (51), it has been very rare, and spectinomycin-resistant N. gonorrhoeae was not isolated in the 2000s (14~17). For this reason, numerous gonococcal infections were treated with spectinomycin in Korea during the 2000s. However, recent changes in sexual behavior may have caused treatment failure in patients with gonococcal pharyngitis who are treated with spectinomycin (68). These patients may serve as a source of dissemination of gonorrhea and provide the means for in-vivo intragenic transfer in PBP2 between N. gonorrhoeae and other commensal Neisseria species (58).
Conclusion
In Korea, the antimicrobial resistance of N. gonorrhoeae is very severe and most isolates are multi-drug resistant to penicillin G, tetracycline, and fluoroquinolones. The incidence of PPNG decreased significantly, but the incidence of TRNG increased recently. The MICs of ceftriaxone were within the susceptible range for all isolates, but MIC creep was apparent and one cefixime non-susceptible isolate (0.5 µg/ml) was found. Almost all isolates were susceptible to spectinomycin, but caution should be required when dealing with gonococcal pharyngitis.
 XML Download
XML Download