

 PDF
PDF ePub
ePub Citation
Citation Print
Print


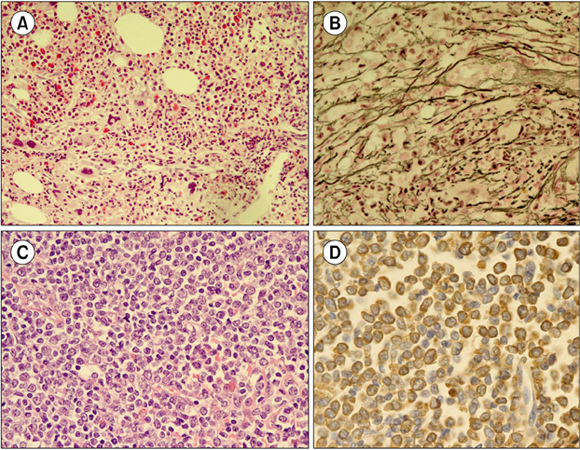
A 54-year-old man was referred to our hospital with right flank pain. Three years ago, he was diagnosed with gastric mucosa-associated lymphoid tissue (MALT) lymphoma and successfully treated with radiotherapy. CBC showed a WBC count of 24.12×109/L (70% neutrophil, 14% lymphocyte, 4% monocyte, 2% eosinophil, 1% basophil, 4% metamyelocyte, 5% myelocyte, and 1/100 WBCs normoblast); Hb level, 10.2 g/dL; and platelet count, 416×109/L. Bone marrow (BM) examination showed granulocytic and megakaryocytic proliferation with moderate dysplastic megakaryopoiesis (A; H&E stain, ×200), and diffuse reticulin fibrosis (B; reticulin stain, ×400). Primary myelofibrosis was the first diagnostic consideration after BM study. Chromosomal analysis, however, showed t(9;22)(q34;q11.2), indicating CML. Concurrent abdomen computerized tomography revealed enlarged inguinal lymph nodes. Inguinal lymph node biopsy showed diffuse infiltration of immature cells (C; H&E stain, ×400), which were positive for myeloperoxidase (D). BCR/ABL1 rearrangement was demonstrated by fluorescence in-situ hybridization analysis, and a diagnosis of granulocytic sarcoma (GS) was made. Accompanying extramedullary myeloid tumor, CML was classified as blastic phase. Secondary CML with a simultaneous manifestation of GS is rare. Combining morphological and molecular-cytogenetic approaches can help detect the coexistence of both neoplasms, especially in CML cases with fewer typical morphologic features.
 XML Download
XML Download