

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately one-third of non-Hodgkin's lymphoma (NHL) arises in tissues other than the lymph node, spleen, or thymus; such lymphomas are termed as primary extranodal NHL [1]. The study of extranodal lymphomas as a group, with regard to etiopathogenesis, biologic features, clinical characteristics, and outcome, has been the subject of several publications [2-5]. According to previous studies, it has been claimed that nodal and extranodal lymphomas have a separate genetic origin and it has been suggested that these forms should be regarded as separate nosological entities [5-11].
Computed tomography (CT) scanning is the current approach used for initial staging and evaluation of response to therapy for lymphoma over the last 2 decades. More recently, there have been significant advances in cancer imaging techniques. Cancer imaging by positron emission tomography (PET) using 2-[fluorine-18]fluoro-2-deoxy-D-glucose (FDG) is based on the observation that most cancers, including lymphomas, metabolize glucose at an abnormally high rate. Further, abnormal FDG uptake measured by the maximum standardized uptake value (SUVmax) is correlated with cellular metabolism and can be influenced to some degree by the cell cycle speed [12, 13]. Recent studies showed that the maximum tumor diameter (MTD) of conventional CT was an adverse prognostic factor, and SUVmax of 18-FDG PET might have potential therapeutic and prognostic implications [14-17]. However, studies on SUVmax and MTD in primary extranodal diffuse large B cell lymphoma (DLBCL) are somewhat limited in comparing nodal DLBCL.
The objective of the present study is to investigate whether FDG uptake and MTD have a major impact on the clinical outcome in primary extranodal DLBCLs.
Go to : 
MATERIALS AND METHODS
1. Subjects and design
Seventy-six primary extranodal DLBCL cases in the Pusan National University Hospital from October 2005 to November 2010 that had undergone an initial 18-FDG PET/CT and conventional CT scans of the neck, chest, abdomen, and pelvis for staging were studied retrospectively. All patients were >18 years at diagnosis and were treated with 6 or 8 cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone) therapy. All patients had stage IE or IIE disease according to the Ann Arbor staging system.
2. Definition of primary extranodal DLBCL and exclusion criteria
Lymphoma presenting in extra nodal organs without or with only minor lymph node involvement was considered primary extranodal DLBCL [18]. Patients with involvement of the spleen or thymus were excluded because these sites were defined as nodal location, while patients with bone marrow involvement were also excluded because involvement of bone marrow other than other extranodal sites usually have poorer prognosis.
3. Definition of MTD
For any axes documented with CT, MTD was the longest for tumors involved at extranodal sites [14].
4. 18-FDG PET/CT scanning
All patients underwent initial staging via 18-FDG PET/CT, and some were checked again at response evaluation. Dual-modality PET/CT tomography was performed using a biograph (Siemens Medical Solution, Hoffman Estates, IL, USA) based on a dualslice helical CT and full-ring PET. FDG PET images were analyzed by the associated nuclear physicians after intravenous administration of 3-6 MBq/kg of 18F-FDG and were displayed with rotating projection and in axial, coronal, and sagittal planes. FDG-PET images were evaluated for regions of focally increased tracer uptake. In the target lesions of FDG tracer uptake, an SUV ≥2.5 as a contouring border was considered to represent lymphoma, as suggested by Freudenberg et al. [19]. CT images were then used for attenuating the correction of PET. Imaging reconstruction of corrected emission data was performed after Fourier transformation with AWESOME algorithm (2 iterations, 8 subsets, and 5-mm Gaussian filter) [20]. CT parameters were set to 130 mA, 130 kV, and a slice width (or 5 min and table feed) of 8 mm per rotation. Intravenous or oral contrast agents were used, and a standardized breathing protocol was applied.
5. Response evaluation
CT scans were documented after 3 and 6 cycles of R-CHOP, and revised response criteria described by Cheson et al. were used [21]. Complete remission was defined as disappearance of all evidence of disease, and partial remission was defined as at least 50% regression in the sum of measurable disease and no involvement of a new site. Relapse disease or progressive disease was defined as any new lesion occurring or a lymph node/extranodal site with a short axis diameter of <1.0 cm increasing by ≥50% and to a size of 1.5×1.5 cm or more than 1.5 cm in the long axis and at least a 50% increase in the longest diameter of any single previously identified node/extranodal site >1 cm in its short axis. Stable disease was defined as failure to attain CR/PR or PD.
6. Statistical analysis
Progression-free survival was defined as the length of time from remission to being worse, and overall survival was defined the length of time from diagnosis to death. SUVmax and MTD are quantitative variables. The cut-off values were decided by analyzing different cut-off levels between the 25% and 75% quartiles by using the log-rank test. Kaplan-Meier curve was used for the survival analyses. A log-rank test was used for comparing significance between different survival curves. Multivariate analysis was performed using the Cox regression model for those factors, which had confirmed significance in univariate analysis. All the data were entered and analyzed using SPSS (SPSS Inc., Chicago, IL) 17.0 for Windows, and P value<0.05 was set as statistically significant.
Go to :
RESULTS
1. Patient characteristics
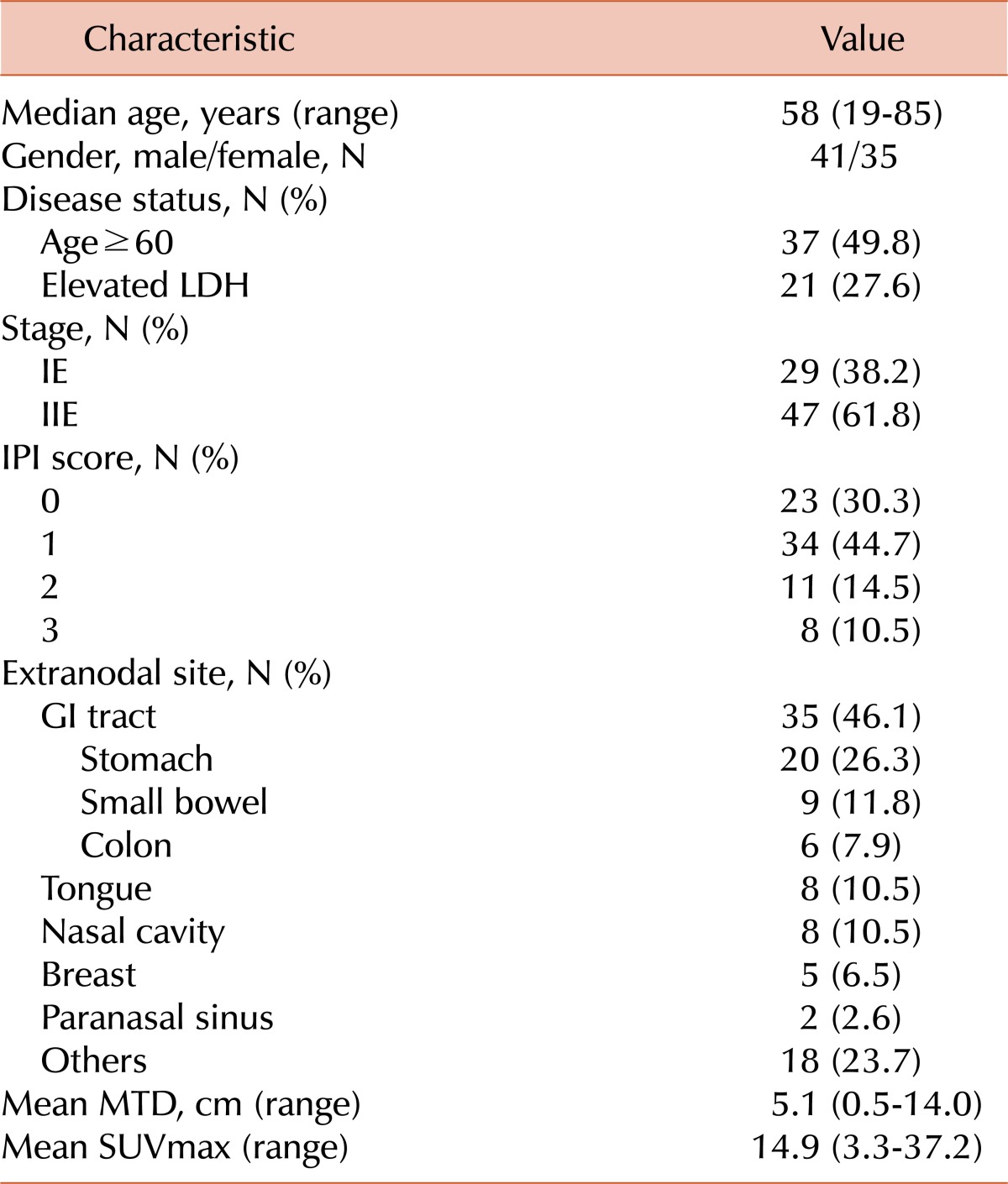
The patient characteristics are shown in Table 1. The mean age was 58 years (range, 19-85), and 37 patients (49.8%) were >60 years old. According to the Ann Arbor staging, 47 patients (61.8%) had stage IIE and 29 (38.2%) had stage IE. Mean follow up period was 35 months. At the end of the follow-up, progression-free survival (PFS) and overall survival (OS) were 73.5% and 76.4%, respectively. International Prognostic Index (IPI) score was distributed from 0 to 3 because all patients had stage IE or IIE and 1 extranodal site involvement; 57 patients (75%) had an IPI score of 0 and 1. Extranodal involvement included GI tract (N=35), tongue (N=8), nasal cavity (N=8), breast (N=5), paranasal sinus (N=2), and others such as rib, abdominal wall, and skin (N=18). All patients had a performance status of ≤3. Mean maximum tumor diameter was 5.1 cm (range, 0.5-14), and mean SUVmax was 14.9 (range, 3.3-37.2).
2. Evaluation of cut-off value of SUVmax and MTD for survival
Cut-off value was decided by analyzing different cut-off levels between the 25% and 75% quartiles by using the log-rank test. Cut off values of MTD and SUVmax were 7.5 and 11.0, respectively.
3. Outcome and prognostic indicators of survival
Univariate analysis was performed on parameters with an impact on survival, sex, age, lactate dehydrogenase (LDH), IPI, MTD, and SUVmax. In the univariate analysis, 3 parameters had an impact on PFS and OS, namely IPI, MTD, and SUVmax.
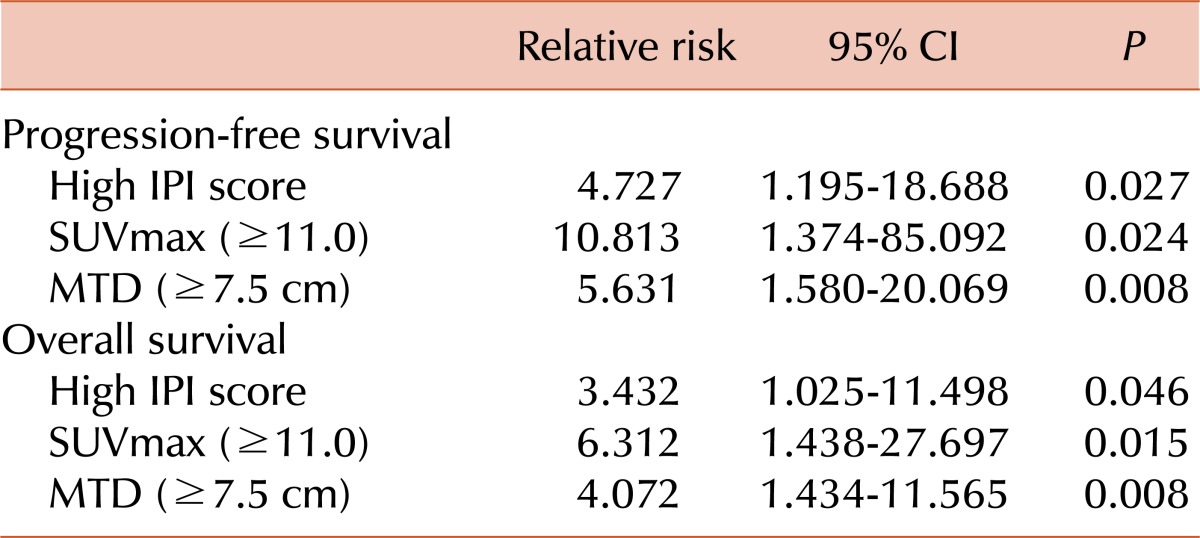
SUVmax of <11.0 predicted longer PFS (P=0.002) and OS (P=0.002). In addition, MTD <7.5 cm also predicted longer PFS (P=0.003) and OS (P=0.003) (Fig. 1). Age and LDH level among IPI factors were not associated with PFS and OS, but IPI was associated with poor PFS and OS. Survival rate was progressively related to IPI (PFS, P=0.001; OS, P=0.000). IPI was classified into high risk (score 3) and low risk (score 0-2), and a IPI of ≤2 predicted longer PFS (P=0.046) and OS (P=0.030) (Fig. 2). In the multivariate analysis with 3 parameters (MTD, SUVmax, and IPI score); all 3 parameters were significantly associated with PFS and OS (Table 2).
 | Fig. 1Progression-free survival and overall survival according to SUVmax and MTD. (A, B) The cut-off value of SUVmax was 11.0. SUVmax more than 11.0 was significantly associated with poor survival outcome (PFS, P=0.002; OS, P=0.002). (C, D) The cut-off value of MTD was 7.5 cm. MTD above than 7.5 cm was also significantly associated with poor survival outcome (PFS, P=0.003; OS, P=0.003).
|

We also evaluated whether the extranodal site of involvement had an impact on survival and ascertained that it was not associated with survival (GI tract, P=0.247; tongue, P=0.466; breast, P=0.870).
Go to :
DISCUSSION
Many factors such as performance status, IPI, B symptoms, and serum β2-microglobulin are indicating factors in the prognosis estimation of DLBCL. Recent studies indicated that bulky mass and high SUVmax could be prognostic parameters suggesting large tumor burden [14-17]. These prognostic factors usually affect both nodal and extranodal DLBCL. However, unlike nodal disease, primary extranodal DLBCL had a separate genetic origin [5-10]. Therefore, the present study evaluated whether these prognostic factors had an impact on survival outcome in primary extranodal disease.
It was reported that MTD had adverse prognostic value in young patients with good-prognosis DLBCL [14]. In this previous study, the cut-off value of MTD was 10.0 cm, whereas in our study it was defined at 7.5 cm, considering the fact that the number of patients with MTD above 10.0 cm was limited in our study. However, adverse prognostic value still existed in both studies.
In the past, the imaging of initial evaluation and follow-up of lymphoma was based solely on the findings of contrast-enhanced CT. However, as contrast-enhanced CT has limited sensitivity in detecting involvement of normal-sized lymph nodes, bone marrow, spleen, and extranodal tissues, 18-FDG PET/CT has been widely used for staging of disease, detection of recurrence, and monitoring of treatment response in patients with Hodgkin disease and NHL [22]. The intensity of FDG uptake in lymphoma is determined by many factors, including viable tumor cell fraction, tumor cell proliferation, upregulation of glucose metabolism, salvage and tumor-specific pathways, and the presence of hypoxia, and suggests large tumor burden [23, 24]. Consequently, initial intensity of FDG uptake was associated with survival outcome, and the cut-off point of SUVmax was considered a poor prognostic factor, which is also a finding of our study. Although there was some evidence that PET/CT is a valuable diagnostic, predictive, and prognostic tool in DLBCL, limitations of 18-FDG PET/CT still remain, including protocol variability by center, easily affected quantification of SUV depending on the time after FDG infusion and blood glucose level, and inconsistency of CT scanning.
Moller et al. showed differences between nodal and extranodal DLBCL [25]. This study announced that patients with extranodal DLBCL in stage I disease were markedly older and had poorer performance status. However, extranodal disease itself was associated with poor survival irrespective of IPI. The relationship among IPI factors such as age and LDH level, sex, and prognosis was also evaluated in stage IE or stage IIE extranodal DLBCL. Only IPI was associated with an inferior survival outcome as a result.
It has been reported that the prognosis according to extranodal site of involvement was not different [19]. However, other studies showed that lymphoma arising in 2 specific sites (Waldyer's ring and GI tract) showed very favorable features at diagnosis, whereas the DLBCL arising in the other areas presented with unfavorable characteristics [11]. Our study indicated that specific site of extranodal involvement was not associated with significant survival outcome, and further studies are required to determine the impact of location or extranodal involvement.
The limitation of the present study was that it was performed retrospectively with small number of patients, and the treatment modalities after R-CHOP chemotherapy, such as radiotherapy and second-line chemotherapy were not analyzed. The 18-FDG PET/CT has some limitations of its own, as mentioned earlier. Further studies about newly emerging parameters such as mean SUVmax, metabolic tumor volume, and tumor glycolysis are needed.
In conclusion, SUVmax and MTD were significantly related to the survival outcome of patients with primary extranodal DLBCL, while high SUVmax (cut-off value 11.0) and MTD (cut-off value 7.5 cm) were poor prognostic factors. More intensive therapy should be considered in patients with high SUVmax and MTD in primary extranodal DLBCL.
Go to :
 XML Download
XML Download