

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Myeloid sarcoma (MS) (initially known as granulocytic sarcoma, and then chloroma) is a rare localized tumor composed of immature granulocytic precursor cells. This extramedullary tumor can affect any organ and can present before, in concurrence with, or after the diagnosis of acute myeloid leukemia (AML) or other myeloproliferative disorders, or as a manifestation of disease relapse [1]. The World Health Organization (WHO) classification recognizes different variants of this tumor based on the predominant cell type and the degree of cell maturation [2]. Extramedullary disease is associated with every cytological subset of French-American-British (FAB) individuals; the disease is frequently found in patients with a monocytic component (FAB M4 and M5), but it is seldom found in patients with acute promyelocytic leukemia (APL) [3].
APL accounts for approximately 10% of AML cases, and is characterized by a favorable clinical outcome [4]. Several types of extramedullary leukemic infiltrates have been reported in APL patients; the skin (leukemia cutis) and the central nervous system (CNS) are the preferred sites of extramedullary involvement in APL. Among primary extramedullary localizations, chloroma is an uncommon pathognomonic lesion, and it is more appropriately termed as promyelocytic sarcoma (PS) when it occurs in this subset of leukemia.
In this report, we present a case of PS that presented as a solitary sternal mass without any clinical evidence of hemopathy. A conclusive diagnosis of PS was made only after local identification of the PML/RARα fusion gene by using fluorescent in situ hybridization (FISH).
Go to : 
CASE REPORT
A 19-year-old man who had a history of asthma and resultant steroid treatment presented with sternal pain, fever, and fatigue in December 2009. Physical examination revealed a solid sternal extramedullary mass with local erythema, and the patient reported persistent pain. Neither trauma nor infection was reported. Magnetic resonance imaging (MRI) scans showed edema, periosteal reaction, and irregular signals from the bone marrow (Fig. 1). Antibiotic therapy was initiated because of the putative diagnosis of osteomyelitis. However, the pain persisted, thereby prompting reevaluation. The blood cell count was normal: hemoglobin, 15.9 g/dL; red blood cells, 5.5×1012/L; white blood cells, 7.4×109/L (with neutrophils, 3.2×109/L; eosinophils, 0.4×109/L; lymphocytes, 2.9×109/L; and monocytes, 0.4×109/L); and platelets, 202×109/L. In March 2010, the patient underwent surgery. A lobulated tumor that was stuck to the sternum but did not infiltrate it was removed during surgery. Complementary biopsies of the sternum and the peri-sternal tissue were performed. Histopathological examination of the tissue revealed an infiltration by myeloid cells, of which some cells had a promyelocytic morphology and contained azurophilic granulations and Auer rods. The immunophenotypic study was limited to specific antigens, but most of the cells did not express CD34. Cytogenetic studies of the PML/RARα fusion gene by using FISH (LSI probe) and PML/RARα dual color probe (Dual fusion translocation probe, Vysis/Abbot) showed t(15;17) (q22;q21-22) (Fig. 2). Diagnostic workup of the patients, including determination of the coagulation profile and assessment of the bone marrow aspirate, yielded normal results, and neither atypical promyelocytes nor blast cells was detected in the peripheral blood and bone marrow. In addition, negative results were obtained in cytogenetic and PCR analysis for PML/RARα transcription in peripheral blood and bone marrow cells. Taken together, the results suggested a diagnosis of PS. The patient was treated in accordance with the French APL-2006 trial: a combination of all-trans retinoic acid (ATRA) (45 mg/m2/day for 30 days), idarubicin (12 mg/m2/day for 3 days), and cytarabine (200 mg/m2/day for 7 days) was administered. Further evaluation of the patient after induction therapy was not possible because of the specific morphological and molecular results at the time of diagnosis. However, the patient still received 2 additional courses of consolidation chemotherapy followed by local radiotherapy in the sternal region, and a 2-year maintenance therapy involving oral administration of 6-mercaptopurine and methotrexate was scheduled.
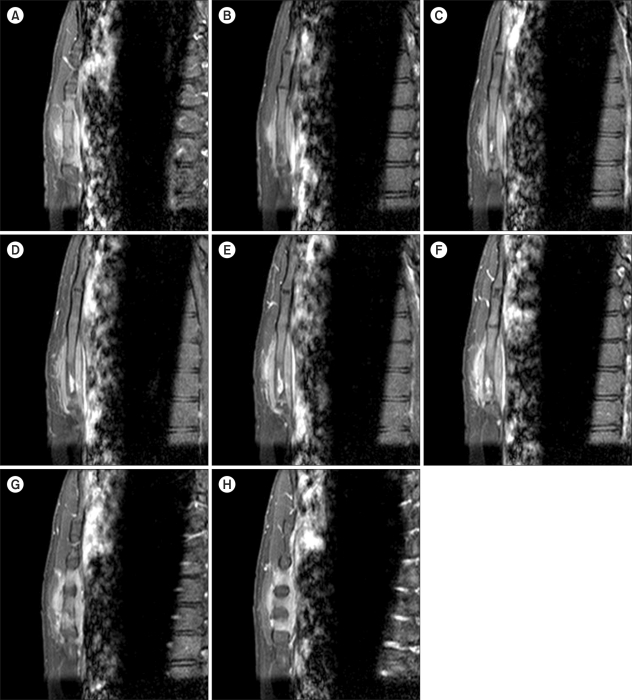 | Fig. 1Magnetic resonance imaging of the sternum. Sagittal-weighted images (A to H) show injury to almost the entire sternum. The sternum shows an obvious abnormality at the distal end with a centro-osseous necrotic mass measuring 24 mm in transverse section, 7 mm in thickness, and 20 mm in height. The soft tissue swelling in the pre- and retro-sternal areas is significant with intense enhancement spanning nearly 50 mm.
|
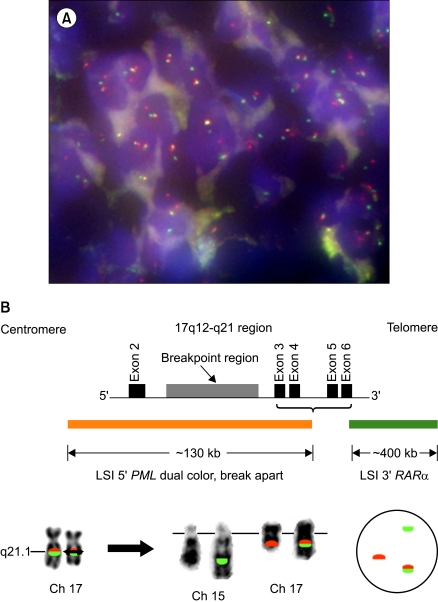 | Fig. 2The reciprocal and balanced t(15;21), involving the PML gene on chromosome 15q22 and the RARα gene on chromosome 17q12.1, is a characteristic molecular feature of APL. In APL cells containing t(15;17), 1 orange (PML), 1 green (RARα), and 1 fusion (PML/RARα) signal pattern is observed (A). Two gene fusion products result from this translocation and encode the functional chimeric proteins: PML/RARα and RARα/PML. The LSI PML/RARα probe is a mixture of 2 FISH DNA probes. LSI PML is labeled in spectrum orange and LSI RARα is labeled in spectrum green (B).
|
Go to :
DISCUSSION
The problems related to the diagnosis and prognosis of MS can be attributed to its clinical mode of appearance. Since most patients never develop systemic disease, a correct and timely diagnosis may be rather difficult. Diagnosis is easier when MS is concomitant with leukemia [5-7], or when MS develops in patients previously treated for leukemia [8]. Diagnosis is more problematic when MS precedes acute leukemia. Cases of MS are often misdiagnosed as other neoplasms, mainly as malignant lymphomas. In the cases of APL, extramedullary disease is generally observed at the time of relapse and presents as a solitary localization or in association with the hematological features of the disease. The occurrence of extramedullary disease in patients with APL has been increasing since the introduction of all-trans retinoic acid (ATRA) therapy [8]. Such findings have raised several questions regarding the use of this therapy; the increase in the occurrence of extramedullary diseases has been linked to a direct effect of ATRA on adhesion molecules, which increases the infiltration capability of blastic cells [9]. The increase in the occurrence of extramedullary disease can also be a consequence of the prolonged survival of patients who receive ATRA [8]. Furthermore, the occurrence of the ATRA syndrome has been recognized to be a significant risk factor for extramedullary involvement at relapse [9].
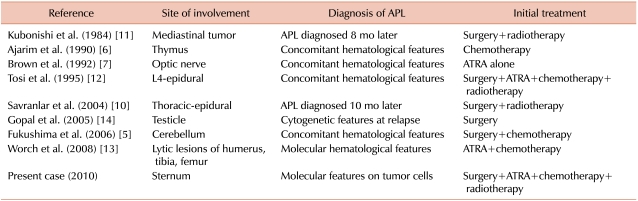
The presence of an isolated localization is much more uncommon in APL at the time of initial diagnosis. In rare cases, MS originates in the subperiosteal regions of the bones (ribs, sternum, or orbital bones) several months before the clinical detection of leukemia, and subsequently spreads to soft tissues. MS can also originate in other regions, such as the spinal epidural space, thereby showing signs and symptoms of spinal compression. PS may have totally gone undetected on initial diagnosis [10-12], and it may actually be diagnosed later with bone marrow infiltration by promyelocytic malignant cells at the time of relapse. PS may be correctly diagnosed initially by identifying the specific translocation and/or molecular rearrangement in the tumor cells and also by assessing the molecular hematological features, even though the bone marrow aspirate does not show any blastic infiltration [13, 14] (Table 1).
A diagnosis of MS is considered as a possible sign of APL. In this report, we report a rare case of MS; diagnosis of the disease was made after surgical intervention and cytogenetic analysis of the tumor cells. Correct and timely diagnosis is a prerequisite for optimal treatment and outcome. Therefore, establishing an accurate histological diagnosis is a fundamental requirement. The optimal management of patients with this form of APL has not been critically assessed. In some MS cases, the patients do not show any clear leukemic transformation in the later stages. However, the consensus is that all patients showing MS should be treated with intensive chemotherapy [15]. When left untreated, most cases progress to overt leukemia; a majority of the cases show AML transformation in about 10 months [10-12, 14]. Similarly, therapy restricted to local procedures increases the risk of systemic disease. Radiation and intensive systemic therapy may therefore certainly be considered [15], and treatment might involve the same chemotherapeutic schedules that are generally used in leukemia with a "classic" presentation. The standard treatment for APL consists of ATRA combined with conventional chemotherapy [4]. Our patient could not be included into the French APL-2006 clinical trial, but he was treated similarly with an induction course combining ATRA with chemotherapy followed by 2 courses of consolidation chemotherapy and a 2-year maintenance therapy. Furthermore, complementary sternal irradiation was scheduled between the consolidation and maintenance phases.
Go to :
 XML Download
XML Download