

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allogeneic hematopoietic stem cell transplantation (Allo-HSCT) is a well-established treatment for several non-malignant diseases, including severe aplastic anemia (SAA), inherited bone marrow failure (BMF) syndromes, immunodeficiencies, and metabolic disorders [1]. Although complete donor hematopoiesis is a desirable outcome of allo-HSCT in malignant disorders, complete replacement of the recipient's hematopoietic system is not considered necessary to improve the underlying disease state in patients with non-malignant disorders. This coexistence of host and donor hematopoietic cells is known as mixed chimerism (MC).
Rates of graft failure and rejection are high in patients with non-malignant diseases [2, 3]. MC has been linked to graft rejection [4, 5], suggesting that early testing for posttransplant chimerism may help to identify patients at increased risk of graft rejection, who may therefore require immunotherapy [6]. Although patients with a significant proportion of host cells are known to be at increased risk of rejection in cases of malignant disease, only a few studies have focused exclusively on children with non-malignant diseases [7, 8]. Furthermore, the utility of chimerism in predicting subsequent transplant outcomes in non-malignant diseases has not yet been established.
The main aims of this study were to identify the variables affecting chimerism and to determine the impact of MC on transplantation outcomes in patients undergoing allo-HSCT for non-malignant diseases.
MATERIALS AND METHODS
1. Patients and donors
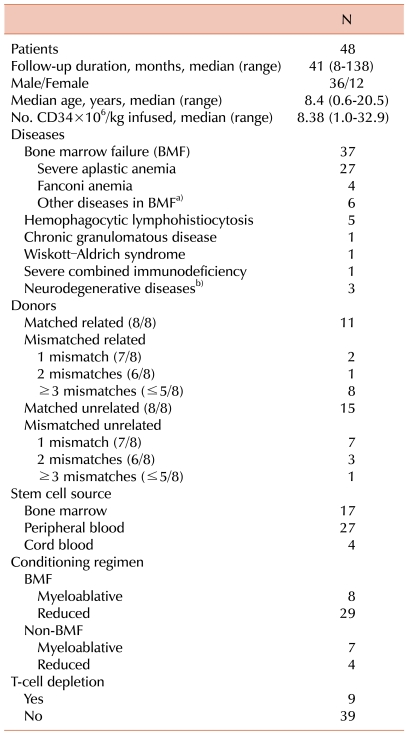
Between April 2000 and March 2011, 48 children underwent 50 allo-HSCTs for non-malignant diseases at the Asan Medical Center Children's Hospital in Seoul, Korea. In this study, we analyzed the initial HSCT data from all patients. Median age at first HSCT was 8.4 years (range, 0.6-20.5 years), and the median duration of follow-up was 41 months (range, 8-138 months). Diseases were classified as BMF or non-BMF. All donor-recipient pairs were fully typed for HLA-A, -B, -C, and -DR using high-resolution molecular typing. As a surrogate marker of iron overload at the time of transplantation, serum ferritin was routinely measured as a part of the pretransplant work-up before the beginning of the conditioning regimen using a 2-site sandwich immunoassay with direct chemiluminescence (ADVIA Centaur, Siemens). All patients were stable, without fever or other events, suggesting that pretransplant ferritin levels are a good estimator of iron status and are not significantly affected by an inflammatory state. Data were analyzed in October 2011. The demographic and clinical characteristics of patients and donors are summarized in Table 1. This retrospective study was approved by the institutional review board at the Asan Medical Center in Seoul, Korea.
2. Graft-versus-host disease
Acute and chronic graft-versus-host diseases (GVHD) were graded according to the established criteria [9].
3. Analysis of chimerism
Whole blood samples were collected from individual donors and recipients at 1 (day 28), 2, 3, 6, and 12 months after allo-HSCT. In cases where MC was detected, chimerism was tested at more frequent intervals. DNA was prepared from whole blood samples using the QIAamp Blood Kit (Qiagen, Hilden, Germany) and quantified spectrophotometrically. Polymorphic short-tandem repeat (STR) markers were amplified using the AmpFlSTR Profiled Plus PCR amplification kit (Applied Biosystems, Foster City, CA, USA). Amplified fragments were analyzed using an ABI PRISM 310 Genetic Analyzer (Applied Biosystems), and peak areas were quantified using Genescan software (Applied Biosystems). The percentages of donor and recipient DNA were calculated from individual proportions of donor and recipient peak areas [10]. Unless otherwise stated, the degrees of STR-PCR and MC were based on host portions.
4. Definition of chimerism and responses
Patients were stratified individually based on serial STR-PCR analyses, with chimerism defined as described previously [7, 8]. Patients with samples showing 1% or less autologous signals after HSCT were classified as having achieved complete donor chimerism (CC). We selected a cutoff of 1%, since microsatellite and several tandem repeat methods have a sensitivity limit of 1-5%. MC was defined as having a recipient fraction of 1% to 99% at any time after HSCT. Patients initially classified as having MC who turned into CC were classified in the transient MC group, while those showing sustained autologous signals greater than 1% were categorized in the sustained MC group. In the sustained MC group, patients consistently displaying autologous signals that did not exceed 30% were considered to have low-level MC, while those displaying a significant increase in autologous cells, up to 30%, were considered to have high-level MC. Patients with more than 99% recipient signals were defined as having attained complete recipient chimerism (RC) or autologous reconstitution.
Since there is no clear consensus on the definition of clinical remission in patients with non-malignant diseases, we assessed the response relative to correction of the underlying disease using disease-specific measures. These included normal hemograms along with transfusion independence in patients with BMF syndromes, immune reconstitution and lack of infection in patients with immunodeficiencies, enzyme concentrations and the results of brain imaging and neurologic examinations in patients with metabolic disorders, and absence of symptoms and discontinuation of pretransplant-specific therapies in patients with autoimmune disorders [11]. A complete response (CR) was defined as a normal hemogram with eradication of the underlying disease. A partial response (PR) was defined as the presence of some positive effects of HSCT, but not fulfillment of the criteria for CR (e.g., patients with BMF that displayed some improvement, but were still transfusion dependent). Disease progression was defined as the absence of positive effects of HSCT.
Graft failure comprises 2 clinical entities: (1) failure to achieve an absolute neutrophil count of 0.5×109/L or less and marrow hypoplasia for less than 60 days with or without the existence of donor-type hematopoiesis, and (2) complete loss of donor-type hematopoiesis occurring anytime after transplantation. Late graft failure was defined as the loss of the graft after engraftment during follow-up.
5. Statistics
The probabilities of overall survival (OS) and event-free survival (EFS) were estimated using the Kaplan-Meier method. An event was defined as graft failure or death either due to treatment toxicity or disease progression. Fisher's exact test was used to compare differences in categorical variables affecting chimerism and response to HSCT between groups, whereas the Mann-Whitney U-test was used to compare continuous variables. We also attempted to model relationships between 2 continuous variables by linear regression. For multivariate analysis, the logistic regression model was used. Rreceiver operating characteristic (ROC) plot analysis was performed to determine the threshold value of CD34+ cells for predicting chimerism. Probabilities of acute and chronic GVHD were calculated using the cumulative-incidence-function method; death without GVHD was the competing event. All statistical analyses were performed using the SPSS statistical program (SPSS Inc., Chicago, IL, USA) or R 2.10.1 software (The R Foundation for Statistical Computing, 2007). All P-values were 2-sided, with P<0.05 considered statistically significant.
RESULTS
Forty-eight patients underwent allo-HSCT, and 2 required a second transplant due to graft failure after the first HSCT. At a median follow-up of 41 months, the 3-year OS and EFS rates were 91.5±4.1% and 85.3±5.1%, respectively. Four patients died, 1 due to graft failure and the other 3 due to transplant-related complications, including veno-occlusive disease, hemorrhage, multi-organ failure, and infection.
1. Chimerism
During follow-up, 23 patients (48%) showed sustained CC and 23 (48%) showed MC. Peak MC in the groups of patients with transient (N=9), low-level (N=10), and high-level (N=4) MC occurred at a median of 3, 3.5, and 2.3 months, respectively. Patients with transient MC achieved CC at a median of 7.7 months after HSCT. All 4 patients with high-level MC showed more than 30% autologous signals within 2 months after HSCT. The chimeric status of patients with high-level MC is shown in Fig. 1.
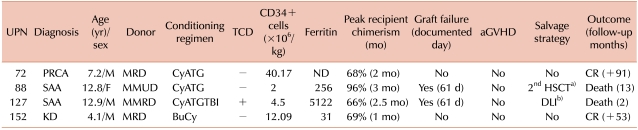
Two of the 4 patients with high-level MC subsequently experienced graft failure after HSCT (Table 2). One of these patients (UPN 88) achieved CR after the second HSCT, but died due to transplant-related complications resulting in multiple organ failure after 5 months. The second patient (UPN 127) received 2 donor lymphocyte infusions (DLIs), but did not achieve stable engraftment, and subsequently died due to infection and pulmonary hemorrhage.
RC was detected on day 28 after HSCT in 2 patients, 1 with hemophagocytic lymphohistiocytosis (HLH) and 1 with SAA. Although the patient with HLH experienced graft failure, BM showed autologous recovery, and the patient remained in CR at data cut-off. The SAA patient achieved neutrophil engraftment on day 11 (10% autologous portion of MC on day 20), but neutropenia occurred at day 14, and STR-PCR revealed 100% host signal at day 28. Owing to graft failure, the patient underwent a second HSCT and achieved CC with stable engraftment.
2. STR-PCR at day 28 post-HSCT
We observed a linear relationship between the degree of day-28 STR-PCR and pretransplant ferritin concentrations. Higher ferritin concentrations were significantly associated with a higher recipient proportion of MC by day 28 after HSCT (r2=0.2, P=0.03). At day 28 after HSCT, STR-PCR values were significantly higher in patients with high-level MC than those with transient or low-level MC (50.8% vs. 3.7%, P<0.01).
We observed a linear relationship between the day-28 STR-PCR and time to engraftment. Specifically, a high proportion of autologous cells at day 28 after HSCT were significantly associated with late neutrophil (r2=0.24, P<0.01) and platelet (r2=0.15, P=0.02) engraftment. No differences were evident in the day-28 STR-PCR between patients with PR and CR. However, STR-PCR at day 28 was significantly lower in the response than the non-response group (6.1% vs. 66.0%, P<0.01).
3. Variables affecting chimerism
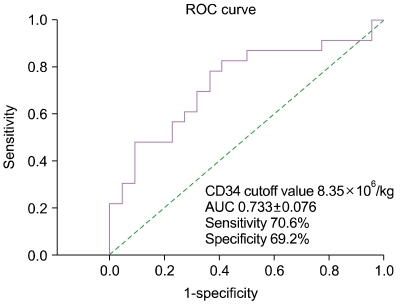
The variables tested for effects on chimerism included patient age, disease category, numbers of infused CD34+ and CD3+ cells, source of stem cells, donor type, degree of HLA match, pretransplant serum ferritin concentration, and intensity of the conditioning regimen. Increasing MC was only observed in patients with BMF. The number of infused CD34+ cells was significantly higher in the CC group than in the MC group (13.2×106/kg vs. 7.2×106/kg, respectively; P<0.01). Similarly, we observed a marked increase in the number of infused CD3+ cells in the CC group compared to the MC group (4.92×108/kg vs. 2.61×108/kg, respectively; P=0.02). The only variable with a significant influence on patients' chimerism status was the number of infused CD34+ cells, as determined by multivariate analysis. Using ROC curves, the optimal cut-off value of CD34+ cells for predicting the chimerism status was estimated to be 8.35×106/kg (70.6% sensitivity, 69.2% specificity), indicating that patients who received less than 8.35×106/kg of CD34+ cells are at higher risk of developing MC (Fig. 2).
4. Chimerism and transplantation outcomes
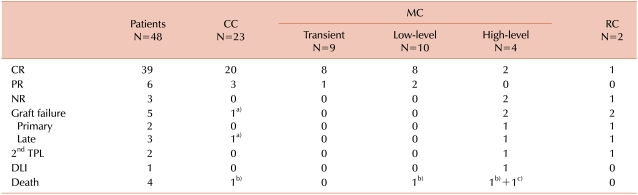
The relationship between chimerism status and clinical response is shown in Table 3. All patients with CC and low-level/transient MC showed clinical responses to HSCT. Among the 23 patients with posttransplant CC, 20 achieved CR, including 1 who experienced late graft failure 39 months after HSCT, but achieved CR after immunosuppressive therapy. The remaining 3 patients achieved PR, 1 each with adrenoleukodystrophy, Krabbe disease, and SAA. Among the 23 patients with posttransplant MC, 21 showed clinical responses to HSCT. Two patients with high-level MC experienced graft failure. The incidence of CR in the transient, low-level, and high-level MC subgroups was 89% (8/9), 80% (8/10), and 50% (2/4), respectively (P=0.03). The incidence of graft failure was significantly higher in the high-level MC subgroup than the low-level and transient MC subgroups (P=0.03). Higher ferritin concentrations before HSCT (P<0.01) and lower numbers of infused CD34+ cells (P=0.01) were additionally associated with graft failure.
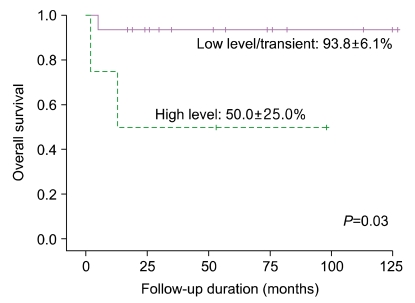
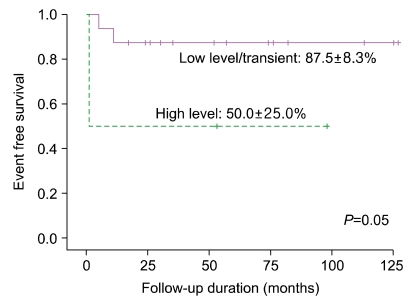
The incidences of grades II-IV acute and chronic GVHD were significantly higher in CC patients than in MC patients (56.5% vs. 13.0%, P<0.01; and 47.8% vs. 21.7%, P=0.04, respectively). No significant differences in survival were evident between the CC and MC groups. However, the OS rate was significantly lower in patients with high-level MC than in patients with low-level and transient MC (50.0% vs. 93.8%, P=0.03; Fig. 3). The EFS rate of patients with high-level and low-level/transient MC was 87.5% and 50.0%, respectively (P=0.05; Fig. 4). The causes of death in the high-level MC group included graft failure and multi-organ failure after second HSCT.
DISCUSSION
This study presents a retrospective analysis of chimerism status and the effects of chimerism on clinical outcomes in children undergoing HSCT for non-malignant diseases. Allo-HSCT was considered the only curative approach for non-malignant diseases in our patients. In our cohort of 48 patients receiving 50 allo-HSCTs, 5 showed graft failure. The overall survival rate was 91.5%, similar to that reported in earlier studies involving patients with non-malignant diseases [2, 12].
Unlike hematologic malignancies, where 100% donor engraftment is always desired, the number of donor cells required for sustained engraftment and correction of underlying disease in patients with non-malignant disorders may be host- and disease-specific. The incidence of MC in our study was 48%, similar to that reported previously [13]. Possible factors associated with MC development include the source of hematopoietic stem cells, intensity of the conditioning regimen, composition of the hematopoietic graft, and type of donor [14-16]. In our experiments, the only variable that had a significant influence on the achievement of MC was the number of infused CD34+ cells, as determined by multivariate analysis. Baron et al. [17] suggested that more rapid reconstitution of the T-cell system and reduced rejection rates could be achieved by increasing the dose of CD34+ cells administered. Similar findings have been reported in other studies [18, 19].
While no significant differences were evident in transplant outcomes between patients with MC and those with CC, acute and chronic GVHD rates were lower in the MC group. Furthermore, all patients with low-level or transient MC successfully maintained engraftment and showed clinical responses to HSCT. The lower incidence of GVHD in the MC group may be attributed to a decrease in alloreactive T-cells that attack recipient tissues or an imbalance between pro-inflammatory and immune-modulating cytokines [20].
STR-PCR at day 28 after allo-HSCT had a predictive value for transplantation outcomes. The degree of STR-PCR was significantly lower in responders than nonresponders. Moreover, day-28 STR-PCR facilitated the identification of patients at risk of high-level MC. Therefore, the degree of chimerism at day 28 after allo-HSCT may be used as a novel platform for additional therapy to induce CR.
High-level MC is correlated with an increased risk of graft failure and rejection [21]. Although we observed no significant differences in survival between the CC and MC groups, we found that patients with high-level MC displayed a higher rate of graft failure and lower survival than those with low-level or transient MC. MC is not necessarily associated with graft rejection, but patients with more than 30% recipient cells in serial samples may be at a higher risk of graft failure. However, no graft loss was observed in 50% of patients with increasing MC. Thus, the risk of graft rejection after allo-HSCT may be limited to the period before the development of tolerance, suggesting that chimerism testing is not predictive of rejection once tolerance to donor cells has been established. Our understanding of tolerance development following allo-HSCT for non-malignant diseases is still incomplete.
In patients undergoing allo-HSCT with either myeloablative conditioning or reduced intensity conditioning for hematologic malignancies, elevated pretransplant serum ferritin concentration, a surrogate marker of iron overload, has been associated with lower OS and increased nonrelapse mortality [22-24]. We observed an association of pretransplant ferritin concentration with day-28 STR-PCR, but not chimerism status thereafter, during the first year after HSCT. Patients experiencing graft failure displayed extremely high ferritin concentrations. Iron overload is known to be associated with free radical generation and tissue damage [23]. Overloaded iron may have accumulated in the BM, resulting in deterioration of microenvironmental functions. However, the number of patients with graft failure was relatively small, suggesting the need for larger-scale studies.
Our study had some limitations. First, the retrospective study design, small sample size, and heterogeneous diseases, and transplantation procedures may have precluded meaningful analyses. Nevertheless, this was a relatively large-scale investigation of this rare disease state in children, managed uniformly in a single center. Next, we did not evaluate lineage-specific chimerism in individual patients. Finally, since treatment was based on individual clinical situations, we did not analyze what interventions may have been prompted by the results of chimerism assays, thus affecting patients' clinical outcomes.
In summary, our findings suggest that posttransplant MC in non-malignant diseases indicates a tolerant state associated with decreased incidence of acute and chronic GVHD. MC may thus be sufficient to cure non-malignant disease. However, patients subsequently presenting with more than 30% recipient cells in serial samples may be at a higher risk of graft failure. The degree of chimerism at day 28 after HSCT may allow the prediction of subsequent clinical responses to HSCT. Our findings collectively highlight the potential value of serial chimerism assays combined with clinical evaluation in providing information on transplantation outcomes.

 XML Download
XML Download