

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Low-grade non-Hodgkin's lymphoma (NHL) is a B cell malignancy characterized by an indolent clinical course and long survival [1]. However, low-grade NHL frequently follows a recurrent course that can become refractory to conventional treatment over time, resulting in an incurable disease [2]. Therapeutic approaches for low-grade NHL are still evolving and depend on the extent of initial disease and treatment responses, which tend to be highly individualized [3]. Low-grade NHL presents as a disseminated disease in 10-30% of cases at the time of diagnosis and relapses to involve distant sites after local therapy [4-6]. Therefore, an effective form of systemic combination therapy is important for patients with advanced stage low-grade NHL.
The response rate, progression-free survival (PFS), or overall survival (OS) of patients treated with anthracycline-containing regimens is not significantly better than those of patients receiving a single alkylating agent or a cyclophosphamide, vincristine, and prednisone (CVP) regimen for treating low-grade NHL [7-9]. Fludarabine is a purine analogue and is one of the most effective drugs for treating low-grade NHL; fludarabine-treated patients exhibit better PFS than CVP-treated patients [10]. Fludarabine combined with mitoxantrone, cyclophosphamide, and rituximab have synergistic effects in sensitizing drug-resistant lymphoma cell lines to cytotoxic chemotherapy in vitro [11, 12]. To improve the efficacy of fludarabine as a single agent, various combination therapies have been reported to achieve excellent anti-tumor effects and are comparable or superior to fludarabine alone [13]. Fludarabine combination chemotherapy improves clinical response to 70-90% and prolongs PFS in patients with newly diagnosed, relapsed, or refractory low-grade NHL [14-16]. However, there are some limitations to apply fludarabine combination chemotherapy for treating indolent lymphoid malignancies; in particular, this regimen has no survival benefit, causes long-lasting myelosuppression, and increases the risk of opportunistic infections [17, 18]. Brown et al. assessed cases of advanced marginal zone B cell lymphoma and concluded that fludarabine combination chemotherapy is unsuitable due to significant hematologic toxicity and increased risk of infections, both during and after therapy [17]. In contrast, others have advocated the superior efficacy of fludarabine combination chemotherapy with mild toxicities [19, 20].
Therefore, we assessed the clinical efficacy and toxicity of fludarabine combination chemotherapy for treatment of patients with low-grade NHL.
Go to : 
MATERIALS AND METHODS
1. Patients
Between January 2004 and May 2010, 25 previously untreated patients with low-grade NHL were enrolled in the study. Patients who met the following criteria were considered eligible for inclusion in the study: ≥18 years of age; Eastern Cooperative Oncology Group (ECOG) performance status <3; pathologically confirmed follicular lymphoma, small lymphocytic lymphoma, or marginal zone B cell lymphoma; Ann Arbor stage of non-continuous II or III-IV disease potentially incurable by local radiation therapy; and at least 1 measurable tumor mass on a conventional computed tomography (CT) scan. Exclusion criteria were as follows: previous exposure to a purine analogue; typical chronic lymphocytic leukemia; HIV-positive status; history of malignant diseases; ECOG ≥3; renal and/or hepatic function >2× the upper normal limit; or stage I or II NHL with asymptomatic disease.
2. Treatment
Twenty-two patients were treated using FND chemotherapy (fludarabine, 25 mg/m2 daily for 3 days; mitoxantrone, 10 mg/m2 on day 1; and dexamethasone, 20 mg/m2 daily for 5 days, every 4 weeks); 2 patients were treated using FCM chemotherapy (fludarabine, 25 mg/m2 daily for 3 days; cyclophosphamide, 200 mg/m2 daily for 3 days; and mitoxantrone, 8 mg/m2 on day 1, every 4 weeks); and 1 patient received FCM with rituximab (375 mg/m2 on day 1). Subsequent cycles of chemotherapy were administered, if patients fulfilled the following criteria: neutrophil count >1.0×109/L; platelet count >75×109/L. In patients not achieving these criteria at 4 weeks, treatment was delayed for up to 2 weeks and restarted at the initial dose. If the neutrophil count 2 weeks later was <1×109/L or the platelet count was <75×109/L, the following cycle was administered at 75% of the initial dose after the neutrophil and platelet counts recovered. Granulocyte-colony stimulating factor (G-CSF) was administered in patients with neutropenia grade 3 or higher. Toxicity was evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE; version 3.0).
3. Assessment
Tumor assessments were based on a CT scan of the neck, thorax, abdomen, and pelvis. Treatment response was assessed at 4 weeks after 3 or 4 cycles of primary chemotherapy, if there was no evidence of disease progression. Patients who achieved partial (PR) or complete remission (CR) received additional cycles of chemotherapy (the same regimen). If patients with stage II NHL improved, the primary lesion within the radiation field was treated by involved field radiation therapy (IFRT). A follow-up CT scan, blood count, and chemistry profiling for tumor response after treatment was performed 4 weeks after the last treatment, every 3 months for the first year, every 6 months for the next 2 years, and yearly thereafter until relapse. Response was assessed using the revised response criteria for malignant lymphoma as described by Cheson et al. [21]. CR was defined as the disappearance of all evidence of disease and PR was defined as a ≥50% decrease in the sum of the product of the diameters of up to 6 dominant masses with no increase in the size of other nodes. Progressive disease (PD) was defined as any new lesion or an increase of ≥50% of previously involved sites from the nadir, and patients not included in any of these categories were considered to have stable disease (SD).
4. Statistical analysis
The primary end-points of the study were the overall response rate (ORR; CR+PR) and toxicities. Secondary end-points included event-free survival (EFS) and OS. EFS was measured from date of study entry to the date of disease progression, recurrence, or death from any cause, and OS was measured from the date of study entry to death from any cause. Survival analysis was performed according to the Kaplan-Meier method using SPSS 17.0 (SPSS, Inc., Chicago, IL, USA).
Go to :
RESULTS
1. Patient characteristics and treatment outcome
Twenty-five patients (9 patients with small lymphocytic lymphoma, 4 patients with follicular lymphoma, and 12 patients with marginal zone B cell lymphoma) were enrolled in this study. The tumors in 12 patients with marginal zone B cell lymphoma were sub-classified as extranodal marginal zone B cell lymphoma (11 patients) including tumors in 6 patients with gastric involvement, or nodal marginal zone B cell lymphoma. The median age was 60 years (range, 35-77 years), with 13 of 25 patients (52%) ≥60 years of age. Seven of 25 patients (28%) with an intermediate-risk follicular lymphoma international prognostic index (FLIPI) and 9 of 25 patients (36%) with a high-risk FLIPI were enrolled in this study. Pre-treatment patient characteristics are summarized in Table 1.
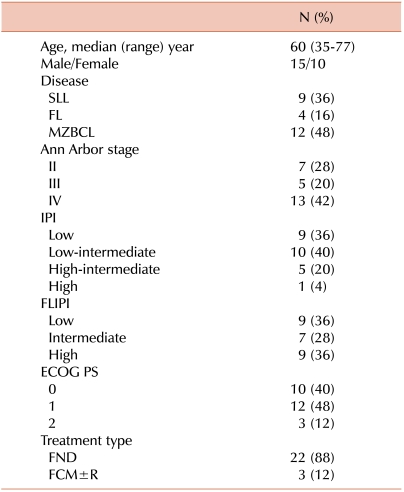
Table 1
Characteristics of 25 patients with low-grade non- Hodgkin's lymphoma.
Abbreviations: SLL, small lymphocytic lymphoma; FL, follicular lymphoma; MZBCL, marginal zone B cell lymphoma; IPI, international prognostic index; FLIPI, follicular lymphoma international prognostic index; PS, performance scale; FND, fludarabine, mitoxantrone, and dexamethasone; FCM±R, fludarabine, cyclophosphamide, and mitoxantrone±rituximab.
![]()
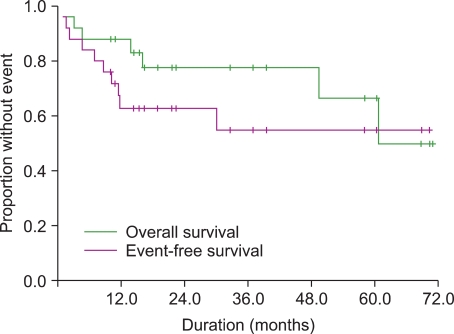
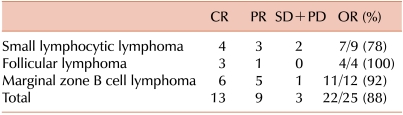
Three patients (12%) had PD after the 2nd cycle of FND chemotherapy; 2 SLL patients exhibited an incremental increase in palpable lymph nodes, and 1 patient with gastric extranodal marginal zone B cell lymphoma developed obstructive symptoms after 2 cycles of chemotherapy; thus, using early CT scans, we confirmed that these symptomatic patients had PD. After 3 or 4 cycles of fludarabine combination chemotherapy, interim ORR was achieved in 22 patients (88% [CR, 36% and PR, 52%, respectively]). At the end of planned chemotherapy, 22 of 25 patients (88%) showed an ORR of 52% (13/25 [CR]) and 36% (9/25 [PR]; Table 2). After a median follow-up of 19 months, 9 patients experienced disease progression, refractory disease, or death; 3 patients had refractory disease during treatment; 5 patients showed disease progression after achieving PR (2 patients) or CR (3 patients); and 1 patient developed a life-threatening intracranial hemorrhage during chemotherapy. Five patients with disease progression and 1 patient with refractory disease received salvage chemotherapy and 2 other patients did not receive additional chemotherapy due to poor general health. One patient showed PR after salvage chemotherapy and was treated using 90Y-Ibritumomab tiuxetan; the other patient achieved CR after salvage chemotherapy. Both patients maintained CR until the final follow-up. During a median follow-up of 19 months, the estimated 2-year EFS was 63±10% (95% CI, 43-83) and the 2-year OS was 78±9% (95% CI, 60-96; Fig. 1).
2. Toxicity
The median number of chemotherapy cycles was 6 (range, 2-9). Four patients received only 2 cycles of fludarabine combination chemotherapy; 3 of the 4 patients could not continue the scheduled chemotherapy due to disease progression. One patient developed unstable angina irrelevant to the infusion reaction after the 2nd cycle of chemotherapy; this patient achieved PR after 2 cycles of chemotherapy and additional chemotherapy was substituted by IFRT.
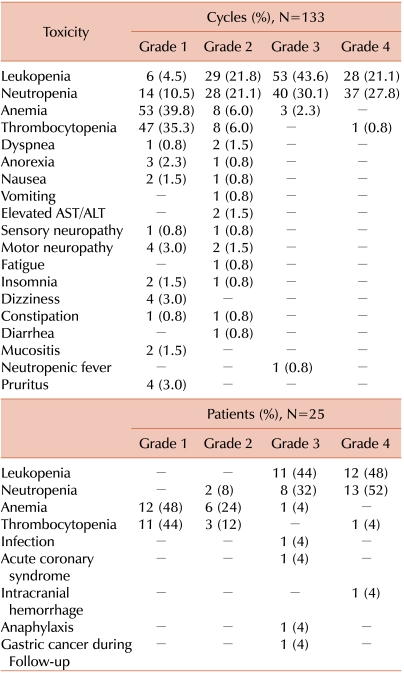
The major toxicities of fludarabine combination chemotherapy were hematologic. A total of 133 cycles of chemotherapy were administered. Grades 3 and 4 leukopenia were observed in 43.6% and 21.1% of the patients, respectively, and grades 3 and 4 neutropenia occurred in 30.1% and 27.8% of the patients, respectively (Table 3). On per patient-treated basis, 52% of the patients experienced grade 4 neutropenia during chemotherapy. Grade 3 or more anemia and thrombocytopenia were rarely observed. Only one (4%) patient developed neutropenic fever during chemotherapy, which improved after subsequent neutrophil recovery. There were no life-threatening infections during fludarabine-containing chemotherapy. In 2 patients (8%), the next scheduled chemotherapy was delayed for 2 weeks due to neutropenia; however, discontinuation of fludarabine-containing chemotherapy due to hematologic toxicities did not occur. Non-hematologic toxicities were generally mild and manageable (Table 3). Grade 3 or higher non-hematologic adverse events developed in 4 patients (16%). One patient developed unstable angina as mentioned, and 1 patient experienced intracranial hemorrhage on day 9 of the 5th cycle; at that time, the patient had a normal platelet count and a normal coagulation profile. During the second cycle of fludarabine infusion, one patient developed grade 3 anaphylaxis with hypotension, skin rash, and fever. This patient was treated using hydrocortisone and anti-histamine, resulting in immediate improvement; thus, the planned chemotherapy was completed without dose reduction. One patient underwent surgical resection due to early gastric adenocarcinoma 36 months after completing fludarabine-combination chemotherapy.
Go to :
DISCUSSION
Conventional therapy for low-grade NHL is based on the use of alkylating agents or combination therapy with or without anthracyclines. Recently, fludarabine, a purine analogue, was actively studied in patients with indolent lymphoma. Over the past 10 years, fludarabine has improved the clinical response and PFS in patients with indolent lymphomas.
We analyzed the safety and clinical efficacy of fludarabine combination chemotherapy for patients with previously untreated stage II-IV low-grade NHL. We showed that ORR was 88% (CR, 52% and PR, 36%) and 2-year EFS was 78%. Thus, the response rate was reasonable in comparison with that obtained using other agents as a first-line treatment for patients with low-grade NHL. CVP and fludarabine monotherapy yielded ORRs of 52-70% and CR rates of 15-39%, respectively, and a median 2-year time to progression rate of approximately 40% [22]. In other studies, the ORRs obtained using fludarabine combination chemotherapy as first-line treatment were 72-94% [23-26]. The high efficacy and long duration of PFS in our study suggest that fludarabine combination chemotherapy is a reasonable option in patients with untreated low-grade NHL.
Hematologic toxicity is a major common complication resulting from using fludarabine as a chemotherapeutic agent. Fludarabine monotherapy has a reported grade 3 or greater neutropenia rate of 23-27% [22, 27]. Combination fludarabine monotherapy with other drugs increased the severity of the neutropenia, particularly when fludarabine was administered in combination with rituximab. Fludarabine combination with rituximab in indolent lymphoma results in grade 4 neutropenia in 36-66% of patients [16, 17, 28], and 27% of patients experienced at least 1 episode of grade ≥3 infection during chemotherapy [16]. We observed that neutropenia is a major problem during chemotherapy. Grades 3 and 4 neutropenia were observed during 30% and 28% of treatment cycles and 52% of patients experienced grade 4 neutropenia during chemotherapy. The association with serious infection during fludarabine combination chemotherapy has been reported with varying incidences. Tam et al. [16] reported that 27% of patients had grade ≥3 infection when treated with fludarabine, cyclophosphamide, and rituximab (FC-R) combination therapy. Ferrario et al. [15] reported 6.3% of patients (4/63) experienced early death during the prolonged post-chemotherapy aplasic phase when treated with fludarabine and cyclophosphamide combination therapy [15]. However, Tobinai et al. [28] showed that only 7% (3/41) of patients developed grade 3 infection with no grade 4 infection with oral fludarabine in combination with rituximab, despite severe neutropenia. In our study, only 1 patient (4%) experienced neutropenic fever without grade 4 infection and no patients required dose modification of chemotherapy or a delay in treatment for greater than 2 weeks. Proper use of G-CSF and selection of patients from a previously untreated group may reduce infectious episodes despite resulting in severe neutropenia. In this study, 2 patients (8%) experienced a delay in the next scheduled chemotherapy for 2 weeks due to neutropenia without dose reduction. The short duration of neutropenia likely influenced the rare occurrence of serious infections. The other most important complication after fludarabine-based chemotherapy is secondary malignancy. One patient developed solid cancer after completing fludarabine combination treatment, but hematopoietic malignancies, such as myelodysplasia or acute myeloid leukemia, were not observed.
In conclusion, fludarabine combination chemotherapy is a highly effective regimen with a high response rate, tolerable toxicities, and long survival in patients with untreated low-grade NHL.
Go to :
 XML Download
XML Download