

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In sepsis, as a lipopolysaccharide (LPS) is systemically released, systemic inflammation develops following elevation of inflammatory cytokines, including tumor necrosis factor-alpha (TNFα), interleukin 1 (IL-1), and interleukin 6 (IL-6), and complement activation [1-4]. Inflammation and coagulation are closely interrelated processes, and numerous plasma factors such as inflammatory cytokines cause hemostatic imbalance. IL-lα, IL-lβ, and TNFα promote coagulation [5]. In addition, infectious agents directly cause endothelial damage, releasing tissue factor (TF) and exposing collagen with consequent deregulated coagulation. Both abnormal fibrin generation and fibrinolysis have been reported in sepsis [6-8]. Disseminated intravascular coagulation (DIC) is a well-known fatal complication of sepsis, in which microvascular thrombosis and subsequent multi-organ dysfunction commonly lead to the death of patients [6].
Thrombin-activatable fibrinolysis inhibitor (TAFI), a 60-kDa glycoprotein zymogen, is the most recently identified coagulation factor [9-13]. Upon activation by thrombin/thrombomodulin, TAFI becomes the active carboxypeptidase B or U form (TAFIa, 35.8 kDa), and modulates fibrinolysis in vivo by cleaving the C-terminal lysine residues from partially degraded fibrin [10, 13]. The reduction of the C-terminal lysine residues could thereby inhibit the amplification of plasminogen activation by tissue plasminogen activator (t-PA). On the other hand, plasmin could also activate TAFI to TAFIa and inactivate TAFI to a 44.3-kDa fragment, depending on the cleavage site [14]. Hence, TAFI can be influenced by both coagulation and fibrinolysis, particularly when hemostasis is interrupted. An interesting characteristic of TAFIa is the rapid irreversible conformational change at 37℃ to an inactive isoform called TAFIai (Fig. 1), which can be measured in plasma [15]. As previously reported, potato tuber carboxypeptidase inhibitor (PTCI) selectively binds to both TAFIa and TAFIai, but not TAFI; thus, it distinguishes the TAFI isomers in plasma [15]. This observation suggests that TAFIai maintains the open active site even in its inactive conformation [15].
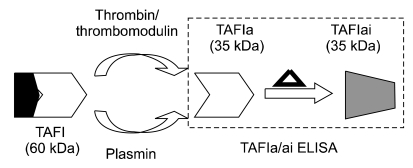 | Fig. 1Thrombin-activatable fibrinolysis inhibitor (TAFI) isoforms in plasma. Thrombin/thrombomodulin or plasmin can activate TAFI (zymogen, 60 kDa), yielding TAFIa (active form, 35 kDa). Subsequently, TAFIa is thermally inactivated (triangle) to TAFIai (shaded). All 3 TAFI isoforms, TAFI, TAFIa, and TAFIai, are found in plasma. TAFIa/ai-specific ELISA measured only TAFIa and TAFIai, not TAFI.
|
Various pathological conditions, including tumor, DIC, deep venous thrombosis (DVT), and coronary heart disease (CHD), give rise to different changes in TAFI levels [16-19]. Elevated TAFI levels were observed in DVT and CHD, which are thought to be caused by increased levels of coagulation factors and consequently increased fibrin clot formation [20, 21]. DIC is also characterized by increased coagulation throughout the body. Reduction of TAFI levels was reported in DIC as well as in sepsis, in which a significant depletion of TAFI was observed in the presence of pathogens in plasma [16]. These results suggest that the consumption of TAFI is an important contributing factor in the pathogenesis of DIC and sepsis. Moreover, in animal models of sepsis using LPS, the supplementation of TAFI was shown to improve the disease outcome; this suggested the therapeutic potential of TAFI [22].
We hypothesized that in sepsis, the consumption of TAFI in zymogen form would result in the accumulation of TAFIa/ai in plasma of sepsis patients analyzed using TAFIa/ai-specific ELISA. We found that the TAFIa/ai-specific ELISA could be a useful assay to observe the elevation of TAFIa/ai in sepsis and could thus be a valuable tool for investigating the role of TAFI and its activation pathway in the regulation of TAFI-dependent fibrinolytic processes.
Go to : 
MATERIALS AND METHODS
1. Plasma samples
Citrated plasma samples from 25 sepsis patients (mean age, 38.4±21.0 years) and 19 healthy individuals (mean age, 42.3±12.1 years) were obtained from Soon Chun Hyang University or Korea University Hospital with informed consent and under the approval from the institutional review board on using the material for this study. Blood was drawn from patients with the salient clinical features of systemic inflammation (fever, tachycardia, tachypnea and/or hypocapnia, and leukopenia or leukocytosis) and a positive culture result for pathological microbes. Plasma was processed as previously reported by centrifugation at 2,000 g for 15 min at 4℃ and subsequent storage at -80℃ before use [15]. Plasma was taken out of the deep freezer before use and thawed on a 37℃ heat block. After 15 min, plasma samples were vortexed and then centrifuged for 5 min at 1,500 g. Prepared plasma was diluted to 30% with Tris-buffered saline with tween-20 (TBST).
2. Materials
Purified human TAFI and anti-human TAFI monoclonal antibodies were purchased from Hematologic Technologies Inc. (Essex Junction, VT, USA). ACTICHROME® TAFI Activity kit, D-phenylalanyl-L-prolyl-L-arginine chloromethyl ketone (PPACK), thrombin and thrombomodulin were obtained from American Diagnostica Inc. (Stamford, CT, USA). Donkey anti-mouse IgG-HRP was obtained from Jackson Laboratories (Bar Harbor, ME, USA). TBST, phosphate-buffered saline pH 7.4 (PBS), and PTCI were purchased from Sigma Chemical Co. (St. Louis, MO, USA). SuperBlock Blocking Buffer, Nunc Maxisorp 96-well black fluorescence microtiter plates, sodium carbonate-bicarbonate buffer (pH 9.4), and ELISA pico-chemiluminescent HRP substrate (ECL solution) were from Thermo Scientific (Hudson, NH, USA). BlockAce was purchased from Serotec (Kidlington, UK).
3. Preparation of TAFIa and TAFIai
TAFI was activated by following the reported protocol [11], which included incubation with α-thrombin (50 units/mL), thrombomodulin (3 units/mL), Ca2+ (5 mM), and TAFI (50 µg) in 500 µL of 100 mM TRIS-HCl pH 7.4 for 20 min at room temperature. PPACK (1 µg) was added to prevent TAFI activation by thrombin. TAFIa carboxypeptidase B activity was examined with ACTICHROME® TAFI Activity assay. TAFIai was generated by incubation of TAFIa at 37℃ for 2 h, completely inactivating the enzymatic activity of TAFI.
4. Specific ELISA for TAFIa and TAFIai
Specific ELISA for TAFIa and TAFIai (Fig. 2) was developed previously on the basis of the selective affinity of PTCI towards the TAFIa and TAFIai isoforms, and not towards the TAFI zymogen form [15]. We measured TAFIa/ai levels in patients with sepsis and healthy controls with TAFIai by using TAFIa/ai-specific ELISA [15]. Fluorescence microtiter plates were coated with PTCI (2 µg/mL) in sodium carbonate-bicarbonate buffer and blocked with SuperBlock Blocking Buffer or BlockAce. The standard curve was generated using twofold serial dilution of TAFIa in phosphate buffered saline (PBS) containing 0.03% Tween 20. The TAFIa, TAFIai, or diluted plasma samples (100 µL) were added to the PTCI-coated plate and incubated for an hour at 37℃ with gentle shaking. After incubation, the plates were washed with TBST 3 times. Anti-human TAFI monoclonal antibody was diluted to 1 µg/mL in TBST. Then, a 100 µL aliquot of mixed anti-human TAFI monoclonal antibody was added to each well and incubated for 1 h at 37℃. Later, the plates were washed again with TBST 3 times. Secondary anti-mouse IgG-HRP (0.1 µg/mL) was added in TBST, and a 100 µL aliquot was added to each well. After 1-h incubation, plates were washed with TBST 3 times, and 100 µL aliquot of ECL solution was added to each well. The relative light unit (RLU) was measured with a PerkinElmer VICTOR3 luminescent microplate reader (Waltham, MA, USA). The standard curve was obtained with serial doubling dilutions of TAFIai, with concentrations ranging from 75 ng/mL to 2.3 ng/mL. The RLU from each TAFIa/ai sample was converted to concentration (ng/mL) using the standard curve (not shown).
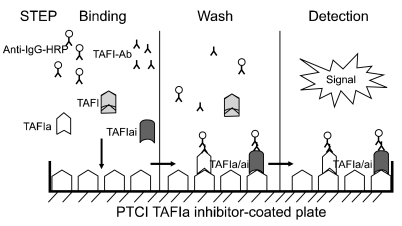 | Fig. 2Schematic diagram of activated and inactivated thrombin-activatable fibrinolysis inhibitor (TAFIa/ai)-specific ELISA. Diluted plasma was applied to a potato tuber carboxypeptidase inhibitor (PTCI)-coated microtiter plate and incubated for an hour at 37℃. Following washes, the TAFIa/ai bound to the PTCI-coated plate was quantitated with anti-human TAFI antibody and horseradish peroxidase (HRP)-conjugated anti-mouse IgG antibody.
|
Go to :
RESULTS
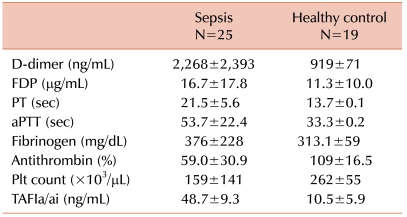
Twenty-five sepsis patients meeting the above criteria were included in our study. The male:female ratio was 1.2:1.3, and median age was 38 years (range, 0-88 years). In all participants, the blood culture was positive, with Escherichia coli being isolated most commonly. Higher levels of TAFIa/ai were detected in plasma samples from sepsis patients than in samples from healthy controls (Table 1). The average values of TAFIa/ai in sepsis and normal plasma samples were 48.7±9.3 ng/mL and 10.5±5.9 ng/mL (P<0.001, Fig. 3) respectively. All samples from sepsis patients showed elevated TAFIa/ai levels than the samples from healthy controls, and the highest value of the healthy samples was 22.7 ng/mL. Because of the limited number of healthy samples, the cut-off value was not set using data from the present study, but a larger number of well-characterized samples from both sepsis patients and healthy donors would provide better assessment of the cut-off values and differentiations. When the levels of TAFIa/ai were compared with other parameters, such as prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen, D-dimer, fibrin degradation product (FDP), antithrombin III, and platelet count, no significant correlation was observed (data not shown). The coefficient of variation (CV) for both inter- and intra-assays from the TAFIa/ai-specific ELISA was less than 10%.
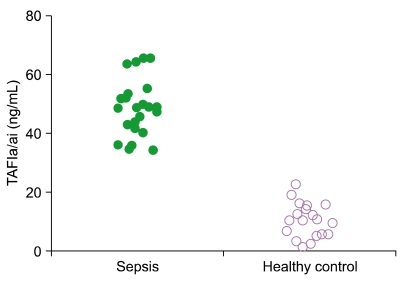 | Fig. 3Quantitation of activated and inactivated thrombin-activatable fibrinolysis inhibitor (TAFIa/ai) levels in plasma from sepsis patients. TAFIa/ai levels were quantitated in 25 plasma samples from sepsis patients (black circles) and in 19 healthy control plasma samples (white circles) using TAFIa/ai-specific ELISA. The average values of TAFIa/ai in sepsis and normal plasma samples were 48.7±9.3 ng/mL and 10.5±5.9 ng/mL (P<0.001), respectively. All sepsis patient plasma samples showed elevated TAFIa/ai levels.
|
Go to :
DISCUSSION
Many studies have correlated diseases with measurements of the total concentrations of TAFI without segregating the following TAFI isomers: TAFI, TAFIa, TAFIai, and 44.3-KDa TAFI. A previous study on hemophilia A reported similar total concentrations of TAFI in hemophilia A patients and healthy controls [23, 24]. On the other hand, the levels of TAFI proenzyme were significantly lower in hemophilia A patients than in controls. In addition, increased levels of TAFIa/ai were reported in hemophilia A patients than in healthy individuals. Since thrombin activation is suppressed in hemophilia A patients, these increased TAFI levels suggested the involvement of plasmin for minimal activation of TAFI in the zymogen form to TAFIa/ai for prevention of bleeding. The results of elevated TAFIa/ai levels in sepsis patientscoincided with the results from a previous hemophilia study [15]. The mean TAFIa/ai antigen levels in hemophilia A samples (88.9±49 ng/mL) is higher than those in samples from sepsis patients (48.7±9.3 ng/mL). Hence, the following hypothesis could be drawn on the basis of the results from both hemophilia and sepsis studies. Instead of measuring total concentrations of TAFI, the zymogen form, or various TAFI isomers, the TAFIa/ai levels could be measured; this would serve as a simple method for monitoring overall changes in TAFI or TAFI activation. Because this method is based on the fact that thrombin/thrombomodulin or plasmin would convert TAFI to TAFIa, and TAFIa would eventually become inactivated to TAFIai, accumulating as an end-product in the TAFI activation pathway. In addition, since the detection of endogenous TAFIa in plasma is rather difficult and TAFIai appears to have a longer half-life than TAFIa in plasma, TAFIai could be an easier target to detect when diagnosing sepsis or hemophilia.
Upon infection, many complex processes, such as activation of the coagulation cascade, neutrophils, proteases, and T-cells, degranulation, release of oxygen free radicals, cytokines, and chemokines, and aggregation of platelets, are involved in sepsis leading to endothelial damage [1]. Inflammation is initiated by cytokines secreted by the phagocytes that recognize pathogens. Cytokines cause vasodilatation and induction of adhesive molecule expression. Monocytes and neutrophils then migrate into the infected tissues. The progress of sepsis eventually leads to coagulation, in which multiple blood coagulation factors involved in both the activation and inactivation of zymogens are simultaneously affected. Since TAFI can be activated by both thrombin and plasmin, TAFI may be involved in numerous pathological conditions, such as tissue inflammation, Budd-Chiari syndrome, hypothyroidism, acute coronary syndrome, rheumatoid arthritis, type 2 diabetes, and hemophilia [23-29]. Hence, TAFI could be a general, but sensitive, marker for monitoring numerous cardiovascular events.
Our results also support the proposal to use TAFI as a therapeutic drug against sepsis. This proposal was based on the findings of studies on sepsis in mouse and baboon models [22]. After the administration of LPS, supplementation of TAFI prevented the dysfunctional response of vascular endothelial cells, similar to the protective mechanism of activated protein C.
In conclusion, the TAFIa/ai-specific ELISA demonstrated higher levels of TAFIa/ai in plasma samples from patients with sepsis than in samples from healthy controls. These results were consistent with those of our previous hemophilia study. The assay was specific for 2 35-kDa activation isoforms of TAFI, namely, TAFIa and TAFIai, but not for the TAFI zymogen. The presence of elevated levels of TAFIa/ai would suggest an up-regulation of the TAFI activation pathway and depletion of TAFI zymogen in both hemophilia and sepsis. TAFIa/ai, measured by TAFIa/ai ELISA, could be used as a novel marker for monitoring perturbation of hemostasis. Monitoring TAFIa/ai antigen levels in plasma would serve as an ideal method to follow the post-treatment progress of recovery from sepsis.
Go to :
 XML Download
XML Download