

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Stent thrombosis (ST) after drug-eluting stent (DES) implantation is a rare, but usually fatal, event leading to acute coronary artery closure that frequently manifests as ST-segment elevation myocardial infarction (MI) or sudden cardiac death. Delayed or absent endothelialization of the stent strut, hypersensitivity or inflammatory reactions to the DES polymer, and the development of neoatherosclerosis within stents with new plaque rupture have been considered as potential causes of late ST occurring with DES.123
The Biolimus A9™-eluting stent (BES; BioMatrix™, Biosensors Interventional Technologies Pte., Ltd, Singapore) is a new generation DES incorporating a stainless steel stent platform and a biodegradable polymer containing the anti-proliferative drug biolimus A9 that is only coated on the abluminal side. The biodegradable polymer could help reduce the risk of late ST, especially in patients with acute coronary syndrome (ACS).456 However, data on the clinical outcome of BES in Korean patients with ACS are scarce. Therefore, the purpose of our study was to determine the effectiveness and safety of the BES in Korean patients with ACS.
Go to : 
MATERIALS AND METHODS
Study design and population
The Biolimus A9™-eluting stEnt in patients with AcUTe coronary sYndrome (BEAUTY) study is a prospective, multi-center, observational study of 1000 ACS patients who underwent implantation of BES at 22 large-volume percutaneous coronary intervention (PCI) centers in Korea.
The inclusion criteria for our study were an age of at least 18 years, presence of ACS, eligibility for PCI with lesions suitable for BES implantation, the presence of one or more de novo stenoses ≥70% in a native coronary artery from 2.25 mm to 4.0 mm in diameter that can be covered with one or multiple stents, and no limitations in the number of treated lesions or number of treated vessels. Unstable angina was considered to be present in patients with ischemic symptoms suggestive of an ACS and no elevation in troponin, with or without ECG changes indicative of ischemia. MI was defined as the third universal definition of MI published in 2012.
The exclusion criteria were patents with other types of DES or bare metal stent (BMS) implantation in a target vessel, chronic renal failure (serum creatinine >2 mg/dL), severe hepatic impairment (serum alanine and aspartate aminotrasferase ≥3 times the upper limit of normal), active bleeding or significant risk of bleeding, or a life expectancy <12 months. We also excluded patients with cardiogenic shock, left main disease, chronic total occlusion (CTO), and saphenous vein graft lesion. Data on baseline clinical, procedural, and lesional characteristics, as well as 1-year clinical outcomes, were collected by a specialized study coordinator at each center using an electronic case report form. The study protocol was approved by the local Institutional Review Board. The approval number was 2011-021 at Chonnam National University Hospital, and all patients provided written informed consent for participation before or after PCI.
Procedure and post-intervention medications
The emergent or early invasive treatments strategies, vascular assess, pre-dilatation or post-dilatation, use of peri-procedural glycoprotein IIb/IIIa inhibitors or anti-thrombotic medication, and complete or culprit only followed by staged PCI for multi-vessel disease (MVD) were determined according to ACS patient status determined at the discretion of operators at each institute. PCI with BES for all lesions was performed in a routine manner. The appropriate length and diameter of the BES, ensuring complete coverage of the lesion, were chosen according to visual estimates by the individual operators. Anti-platelet agents were administered to all patients prior to intervention, including aspirin 300 mg and clopidogrel 300−600 mg or prasugrel 60 mg. After intervention, the patients received aspirin 100 mg once daily indefinitely and clopidogrel 75 mg or prasugrel 10 mg once daily for at least one year. Other medical treatments were also used based on the standard treatment regimen for patients with ACS in a non-restrictive manner.
Study definition
The primary efficacy and safety end point was the incidence of major adverse cardiac events (MACE), defined as a composite of cardiac death, non-fatal MI, and clinically-driven target vessel revascularization (TVR), at 12-month follow-up. Clinically driven TVR was defined as revascularization performed on the treated lesion or vessel of a patient who complained of clinical symptoms, such as chest pain that had increased in frequency, duration, or intensity. ST was defined according to the Academic Research Consortium of Circulatory System Devices Panel Meeting, an advisory committee to the US Food and Drug Administration.
Statistical analyses
The sample size was calculated based on an estimated incidence of MACE of BES in the LEADER study.5 When a two-sided 95.0% confidence interval for a single proportion using the large sample normal approximation extends 0.019 from the observed proportion for an expected proportion of 0.092, the sample size was 889. 10% was added to the sample size to account for possibilities of losses and refusals, resulting in a sampling plan consisting of 1000 patients with ACS. Categorical variables are expressed as frequencies and percentages and continuous variables as mean±SD. The cumulative incidence of clinical events was calculated using the Kaplan-Meier method. Cox regression analysis was used to identify factors affecting the incidence of MACE following the implantation of BES. Only variables with a p value <0.2 in the univariate analysis were included in the multivariate model. Sub-group analyses were performed according to the several clinical status of patients. All the statistical analyses were performed using Statistical Package for Social Science (IBM Corp., Armonk, NY, USA) for Windows, version 21.0.
Go to :
RESULTS
Patient characteristics
Our study enrolled 1000 ACS patients with 1251 lesions between May 2011 and July 2013. Baseline clinical, procedural, and lesional characteristics are shown in Tables 1 and 2. The mean age was 62.6±11.43 years. 72.8% of patients were males, 52.2% had hypertension, 28.5% had diabetes mellitus (DM), and 47.9% presented with acute MI (AMI; ST elevation MI 11.0%, non-ST elevation MI 36.9%). The mean global registry of acute coronary events (GRACE) risk score of all patients was 103.0±27.6. A total of 1300 BESs were implanted in 1251 lesions. In spite of exclusion criteria, some patients with CTO or in-stent restenosis lesions and those with chronic renal failure or left main disease were included (Tables 1 and 2). 51.5% of target lesions were located in the left anterior descending artery, and patients with MVD accounted for 32.8%. 76.4% of total patients received only one stent; one patient received five stents. Most lesions were treated pre-dilatation, although 19.2% were treated post-dilatation. Mean stent diameter per lesion was 3.2±0.44 mm, and mean stent length per lesion 21.4±5.08 mm. Diffuse long lesions (≥25 mm in length) were observed in 22.3% of lesions, and small vessels (≤ 2.75 mm in diameter) were discovered in 23.9% of lesions.
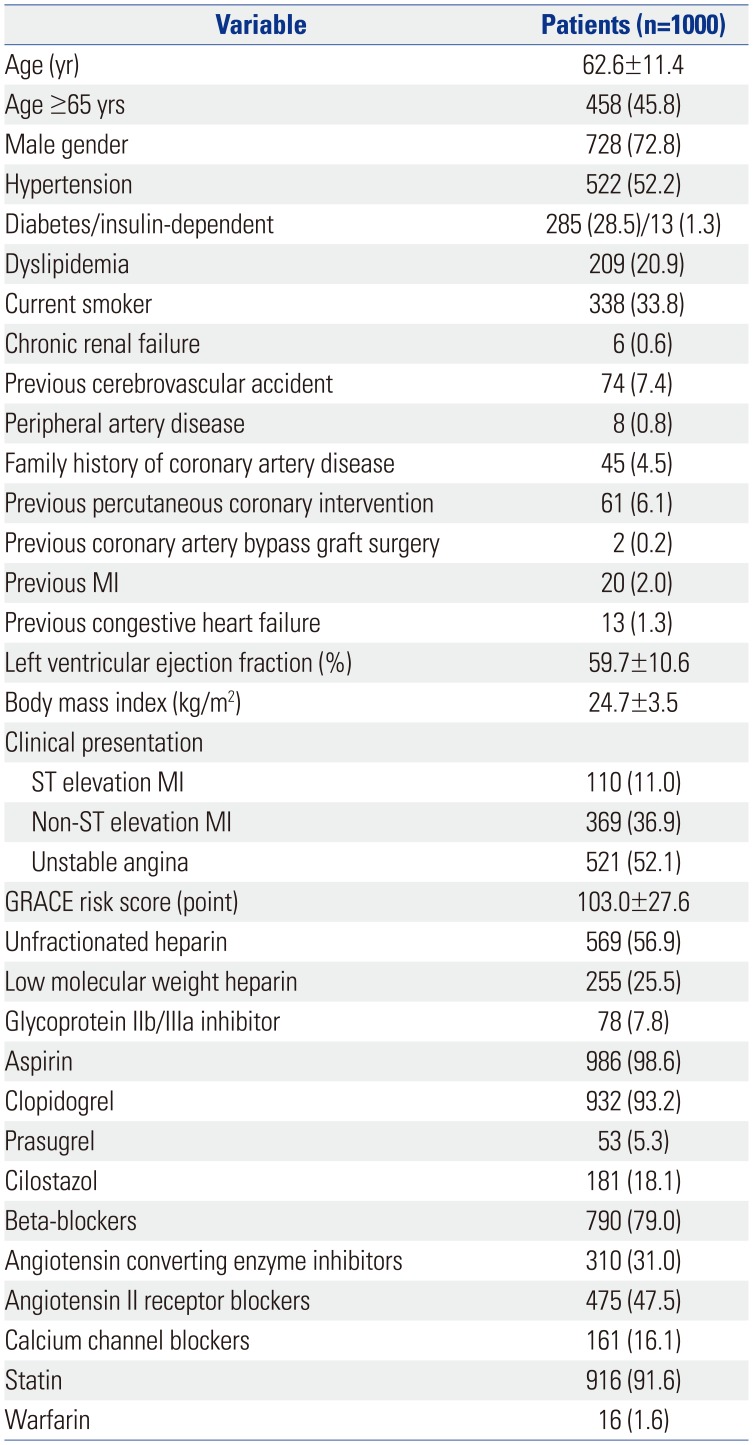
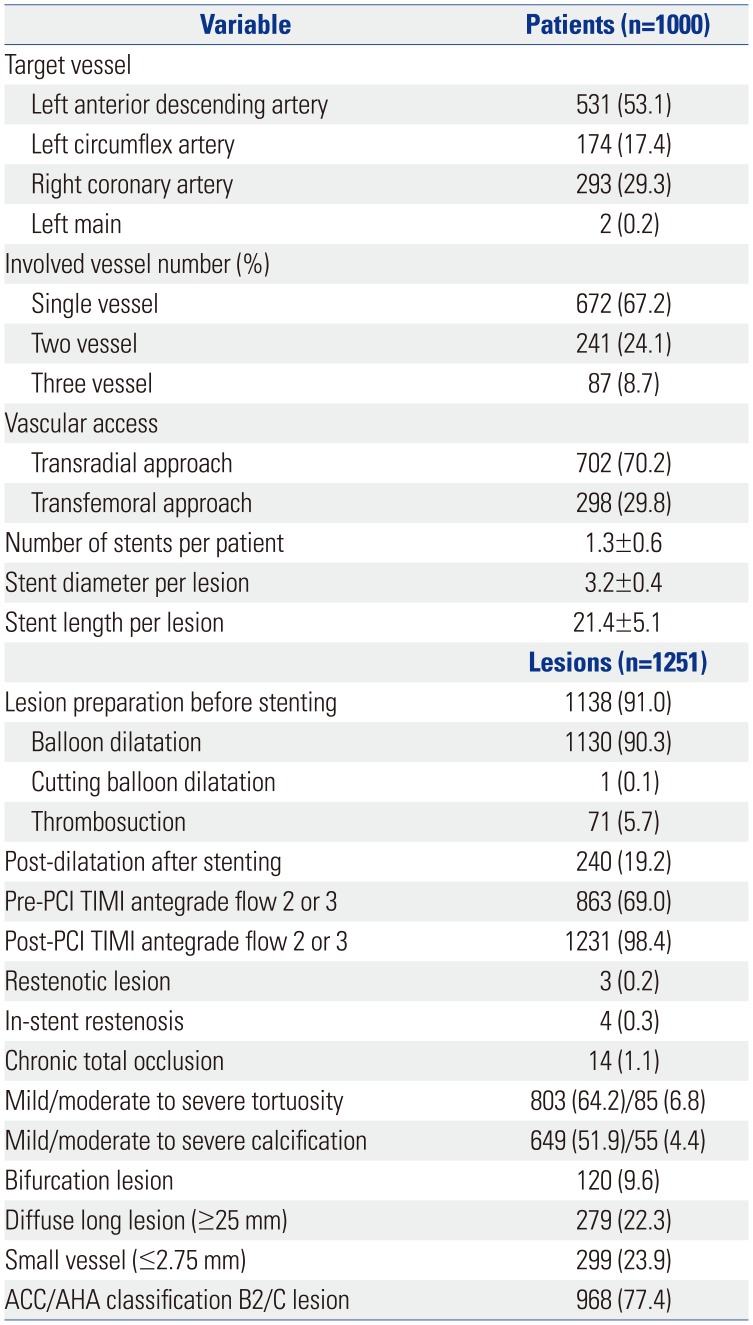
Table 1
Baseline Clinical Characteristics and In-Hospital Medication
![]()
Table 2
Baseline Procedural and Lesional Characteristics
![]()
Clinical outcomes
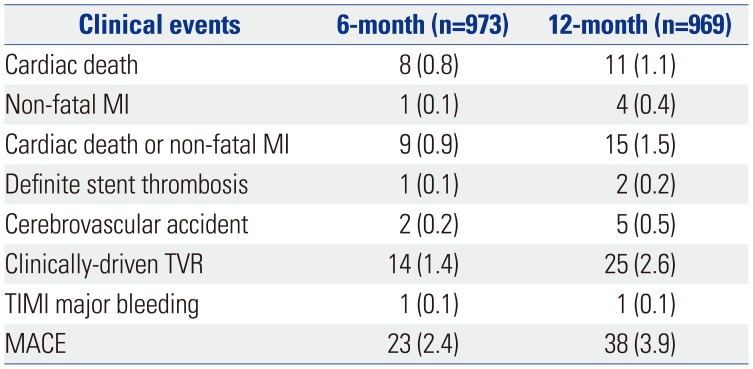
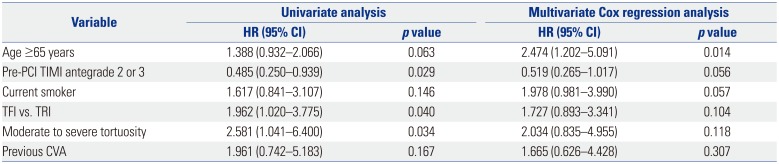
Clinical follow-up was complete in 973 patients at 6 months and in 969 patients at 12 months. 88.6% of all follow-up patients received dual anti-platelet therapy at 6 months and 85.4% at 12 months. The incidence of MACE, a composite of cardiac death, non-fatal MI and clinically driven TVR, at 12-month follow up was 3.9% (Table 3). Cardiac death occurred in 11 patients (1.1%), MI in 4 patients (0.4%), and clinically driven TVR in 25 patients (2.6%), at 12-month follow-up. Two patients suffered from definite ST: subacute (30 days after stent implantation) and late (349 days after stent implantation) ST respectively. Gastro-intestinal bleeding occurred in 1 patient who had received oral anti-coagulant in addition to the dual anti-platelet agents at 6-month follow-up. Kaplan-Meier cumulative event curves at 12 months are shown in Fig. 1. Only age more than 65 years (hazard ratio=2.474; 95% confidence interval= 1.202−5.091) was identified as an independent predictor of 1-year MACE by Cox-regression analysis (Table 4).
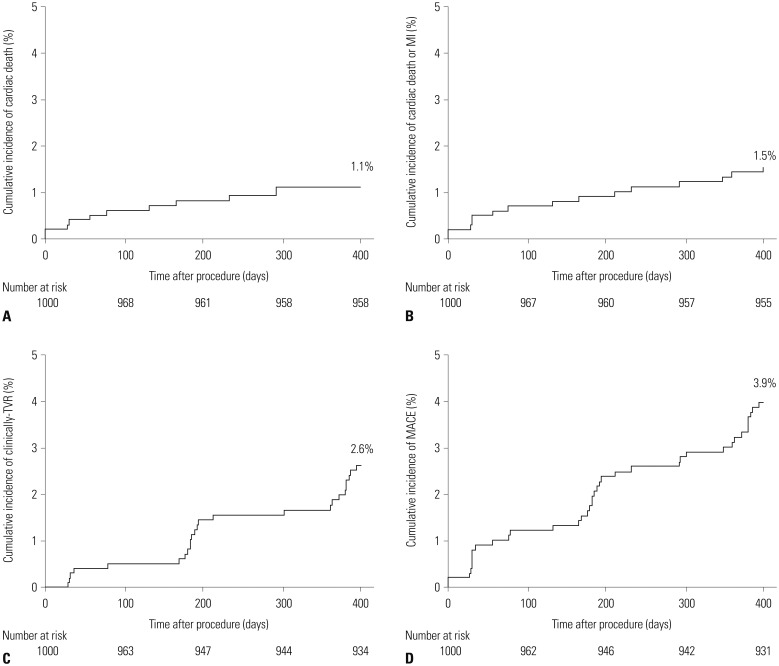 | Fig. 1Kaplan-Meier curves for the cumulative risk of cardiac death (A), a composite of cardiac death or MI (B), clinically driven TVR (C), and MACE (D) at 12 month. MI: myocardial infarction, TVR: target vessel revascularization, MACE: major adverse cardiac events.
|
Table 3
Cumulative Incidence of Clinical Events at 6 and 12 months
![]()
Table 4
Independent Predictors of 1-year Major Adverse Cardiovascular Events by Multivariate Cox Regression Analysis
![]()
Subgroup analyses were performed according to parameters of gender, diabetes status, and presentation with AMI or MVD. Kaplan-Meier cumulative event curves showed no significant differences in the incidence of MACE between males and females (4.1% vs. 3.4%, p=0.593), between patients with and without DM (4.3% vs. 3.7%, p=0.667), between those who presented with AMI and unstable angina (4.4% vs. 3.4%, p=0.403), and between those with MVD and with one vessel disease (4.6% vs. 3.5%, p=0.387) (Fig. 2).
 | Fig. 2Subgroup analyses between males and females (A), between patients with diabetes and without diabetes (B), between patients who presented with AMI and with UAP (C), and between patients with MVD and with 1VD (D). MACE: major adverse cardiac events, DM: diabetes mellitus, AMI: acute myocardial infarction, UAP: unstable angina, MVD: multi-vessel disease, 1VD: one vessel disease.
|
Go to :
DISCUSSION
The present study assessed 1-year clinical outcomes in patients with ACS receiving BES from a large-scale, prospective, real world-registry in Korea. A total of 1000 ACS patients with low GRACE risk scores were enrolled and analyzed. In our results, the incidence of MACE was relatively low and that of definite ST was rare at 12-month follow up. Therefore, our study dem-onstrated that BESs have excellent 1-year clinical outcomes in Korean patients with low-risk ACS.
The BES (BioMatrix® stent) elutes a semi-synthetic sirolimus derivative biolimus A9 from a biodegradable polylactic acid (PLA) polymer, and its platform is composed of stainless steel with a strut thickness of 120 µm.7 Biolimus A9 has a higher lipophilicity and an improved anti-proliferative and anti-inflammatory activity with an enhanced pharmacokinetic profile. The BES, with its asymmetric and abluminal coating, elutes biolimus A9 into the vessel wall, while the PLA polymer is resorbed by tissues. The persistence of durable polymer coatings after completion of the drug release has been implicated as a potential culprit for chronic inflammatory response and related to late ST and restenosis.89 However, the PLA polymer completely resolves into carbon dioxide and water after 6–9 months; therefore, the BES could reduce the risk of ischemic events or ST, especially in patients with ACS, and could shorten the duration of dual anti-platelet therapy after DES implantation.
Many clinical trials have demonstrated BES with biodegradable polymer to be safe and an effective alternative to other DES in patients with coronary artery disease. The safety and efficacy of BES has been established in the LEADERS trial,5 which was a randomized, single-blind, multi-center study comparing a BES with a sirolimus-eluting stent (SES). At 12 months, BES was non-inferior to SES for the incidence of MACE defined as a composite of cardiac death, MI, or TVR, which was 10.7%. In the COMPARE II trial, BES with biodegradable polymer was also shown to be non-inferior to the second generation everolimus-eluting stent (EES) with durable polymer.10 The composite of cardiac death, non-fatal MI, or TVR occurred in 5.2% treated with BES and 4.8% with EES at 12 months. A recently published large-scale network meta-analysis demonstrated that bioabsorbable polymer BESs were associated with superior clinical outcomes, compared with BMS and first-generation DES, and similar rates of cardiac death, MI, and TVR, compared with second-generation durable-polymer DES.11 A cohort study of Korean patients treated with BES (Nobori®) or a zotarolimus-eluting stent showed low incidences of major adverse cardiovascular and cerebrovascular events at 1 year and no significant differences between the two (2.6% vs. 1.7%; p=0.36).12
Our study revealed an incidence of a composite of cardiac death, non-fatal MI, and clinically-driven TVR of 3.9%. It is well known that East Asian patients tend to have a similar or a lower rate of ischemic events after PCI than Western patients, despite a higher level of platelet reactivity during dual anti-platelet therapy.13 Although all ACS patients were enrolled, the incidence of MACE in our study was likely to be somewhat lower than those in LEADERS trial or the other Western studies. This could be explained by ethnic differences and by the fact that we mainly enrolled ACS patients with low GRACE risk scores in our study, excluding those with cardiogenic shock, left main disease, CTO lesions, and graft lesions who are expected to be at high-risk for MACE.
The post-hoc subgroup analysis of our study showed no significant differences in the incidence of MACE based on DM and AMI status. DM is a metabolic abnormality of hyperglycemia and insulin resistance, and exhibits a variety of disease mechanisms, such as abnormal platelet function, coagulation abnormalities, and endothelial dysfunction, that are responsible for accelerated atherosclerosis and the risk of developing coronary artery disease, as well as excessive neointima formation after stent implantation.1415 Therefore, DM is still associated with an increased risk of death, ST, and restenosis after PCI.161718 However, the serial changes of BES in optical coherence tomography analyses showed good apposition and well covered struts at 12 months without a significant decrease in minimum lumen area.19 Experimental studies with a porcine coronary model also showed a lower inflammatory reaction and good endothelialization following implantation of biodegradable polymer BES.202122 These favorable arterial healing findings following BES might lead to improved clinical outcomes in high-risk patients, such as those with DM or AMI, and some studies represented a good clinical outcome of BES in high-risk patients. In meta-analysis with DM patients, biodegradable polymer DESs, compared to durable polymer SES, were associated with comparable overall clinical outcomes during follow-up at 4 years and a significantly lower rate of very late ST (0.4% vs. 2.8%, p=0.02).23 Among patients with ST-segment-elevation MI undergoing primary PCI, BES was as sociated with a low incidence of 1-year MACE (3.2%) and also continued to improve cardiovascular events, compared with BMS beyond 1 year.2425 AMI subgroup analysis of the LEADER trial also showed BES, compared with SES, significantly improved 5-year safety and efficacy outcomes in patients with AMI (18.2% vs. 25.9%, p=0.025).26 Our study will extend the follow-up period of the enrolled patients to 5 years to assess the long-term clinical outcomes of BES in Korean patients with ACS.
In our study, the duration of dual anti-platelet therapy was at least 12 months, in principle; however, 14.6% of all follow-up patients had discontinued the dual anti-platelet therapy within 12 months. The recent trial reported that a short duration (6 months) would be adequate, safe, and effective after implantation of BES.27 That is because the second- and third-generation DESs, especially biodegradable BESs, are likely to present less concerns about ST that occurs as a result of inflammation during healing.2829 However, the optimal duration of dual antiplatelet therapy in patients with ACS, especially AMI, would be different than that in those of stable coronary disease. Therefore, a large, well-designed, randomized trial is needed.
Go to :
Limitations
Our study has several limitations. First, our study did not include all ACS patients and excluded patients with some “off-label” indications. Thus, our results do not reflect real-world clinical outcomes in all-comer high risk patients with ACS. Second, our study was not a randomized, comparative trial and was based on a prospective, observational registry. Therefore, selection bias was not avoidable in the post-hoc sub-group analysis of our study. In addition, we could not evaluate the effect of BES in comparison with that of other DESs in patients with ACS. Third, most of the enrolled patients with ACS were treated with clopidogrel, and therefore, the effect of new P2Y12 receptor inhibitors have been recently used for patients with ACS could not be reflected on our study.
Go to :
Conclusion
Our study demonstrates that BESs have excellent 1-year clinical outcomes in Korean patients with low-risk ACS. The effectiveness and safety of BES appear to be generally consistent for all Korean patients with ACS, regardless of diabetes status and presentation with AMI or MVD. Further large randomized trials are needed, however, to compare clinical outcomes between BES and other DES in Korean patients with ACS.
Go to :
 XML Download
XML Download